

Risk of Severe Non AIDS Events Is Increased among Patients Unable to Increase their CD4+ T-Cell Counts >200+/μl Despite Effective HAART
- PMID: 26020949
- PMCID: PMC4447446
- DOI: 10.1371/journal.pone.0124741
Risk of Severe Non AIDS Events Is Increased among Patients Unable to Increase their CD4+ T-Cell Counts >200+/μl Despite Effective HAART
Abstract
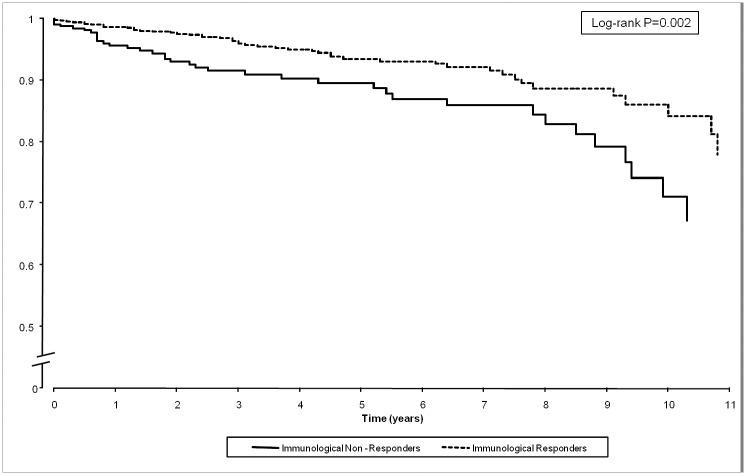
Background: Immunological non-response (INR) despite virological suppression is associated with AIDS-defining events/death (ADE). Little is known about its association with serious non-AIDS-defining events (nADE).
Methods: Patients highly-active antiretroviral therapy (HAART) with <200 CD4+/μl and achieving HIV-RNA <50 copies/ml within 12 (±3) months were categorized as INR if CD4+ T-cell count at year 1 was <200/μl. Predictors of nADE (malignancies, severe infections, renal failure--ie, estimated glomerular filtration rate <30 ml/min, cardiovascular events and liver decompensation) were assessed using multivariable Cox models. Follow-up was right-censored in case of HAART discontinuation or confirmed HIV-RNA>50.
Results: 1221 patients were observed for a median of 3 (IQR: 1.3-6.1) years. Pre-HAART CD4+ were 77/μl (IQR: 28-142) and 56% of patients had experienced an ADE. After 1 year, CD4+ increased to 286 (IQR: 197-387), but 26.1% of patients were INR. Thereafter, 86 nADE (30.2% malignancies, 27.9% infectious, 17.4% renal, 17.4% cardiovascular, 7% hepatic) were observed, accounting for an incidence of 1.83 events (95%CI: 1.73-2.61) per 100 PYFU. After adjusting for measurable confounders, INR had a significantly greater risk of nADE (HR 1.65; 95%CI: 1.06-2.56). Older age (per year, HR 1.03; 95%CI: 1.01-1.05), hepatitis C co-infection (HR 2.09; 95%CI: 1.19-3.7), a history of previous nADE (HR 2.16; 95%CI: 1.06-4.4) and the occurrence of ADE during the follow-up (HR 2.2; 95%CI: 1.15-4.21) were other independent predictors of newly diagnosed nADE.
Conclusions: Patients failing to restore CD4+ to >200 cells/μl run a greater risk of serious nADE, which is intertwined or predicted by AIDS progression. Improved management of this fragile population and innovative therapy able to induce immune-reconstitution are urgently needed. Also, our results strengthen the importance of earlier diagnosis and HAART introduction.
Conflict of interest statement
Figures
References
-
- Paredes R, Mocroft A, Kirk O, Lazzarin A, Barton SE, van LJ, et al. (2000) Predictors of virological success and ensuing failure in HIV-positive patients starting highly active antiretroviral therapy in Europe: results from the EuroSIDA study. Arch Intern Med 160: 1123–1132. - PubMed
-
- Marimoutou C, Chene G, Mercie P, Neau D, Farbos S, Morlat P, et al. (2001) Prognostic factors of combined viral load and CD4+ cell count responses under triple antiretroviral therapy, Aquitaine cohort, 1996–1998. J Acquir Immune Defic Syndr 27: 161–167. - PubMed
-
- Dronda F, Moreno S, Moreno A, Casado JL, Perez-Elias MJ, Antela A (2002) Long-term outcomes among antiretroviral-naive human immunodeficiency virus-infected patients with small increases in CD4+ cell counts after successful virologic suppression. Clin Infect Dis 35: 1005–1009. - PubMed
-
- Loutfy MR, Genebat M, Moore D, Raboud J, Chan K, Antoniou T, et al. (2010) A CD4+ cell count <200 cells per cubic millimeter at 2 years after initiation of combination antiretroviral therapy is associated with increased mortality in HIV-infected individuals with viral suppression. J Acquir Immune Defic Syndr 55: 451–459. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
