

Efficacy of autologous stem cell-based therapy for osteonecrosis of the femoral head in sickle cell disease: a five-year follow-up study
- PMID: 26021713
- PMCID: PMC4465459
- DOI: 10.1186/s13287-015-0105-2
Efficacy of autologous stem cell-based therapy for osteonecrosis of the femoral head in sickle cell disease: a five-year follow-up study
Abstract
Introduction: Stem cell therapy with bone marrow-derived mononuclear cells (BMMCs) is an option for improving joint function in osteonecrosis of the femoral head (ONFH). Bone marrow-derived mesenchymal stromal cell (MSC) numbers and their osteogenic differentiation are decreased in patients with ONFH. However, whether this decrease also extends to the early stages of ONFH in sickle cell disease (SCD) is still unclear.
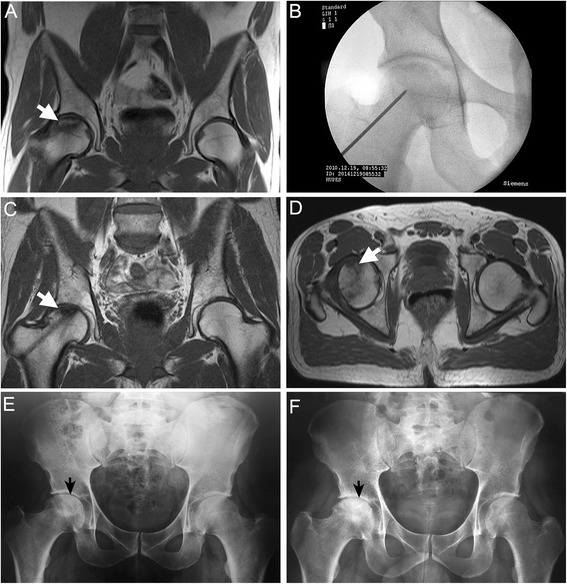
Methods: We conducted a phase I/II, non-controlled study to determine efficacy and safety of BMMC implantation using a minimally invasive technique in SCD patients with ONFH. Eighty-nine patients were recruited and followed up for 60 months after surgery. Clinical and radiographic findings were assessed, and data were completed by in vitro analysis.
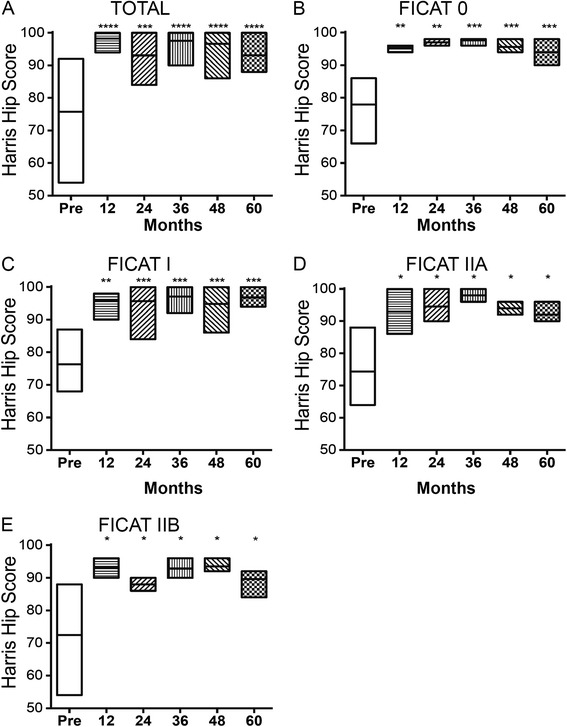
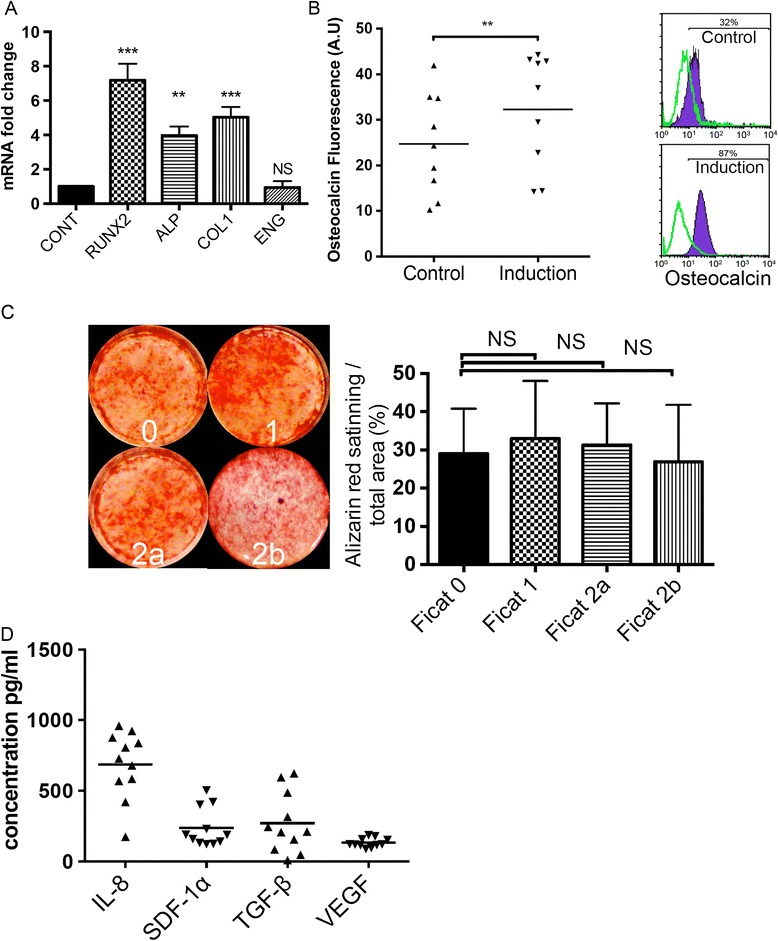
Results: At the final follow-up (60 months) there was a significant improvement in clinical joint symptoms and pain relief as measured by the Harris Hip Score (P = 0.0005). In addition, after the BMMC implantation procedure, radiographic assessment showed disease stabilization and only 3.7 % of the treated patients did not achieve a satisfactory clinical result. The amount of fibroblast colony-forming units was 28.2 ± 13.9 per 1 million BMMCs after concentration. Flow cytometry analysis showed a significantly higher number of hematopoietic stem/endothelial progenitor cell markers in concentrated BMMCs when compared with bone marrow aspirate, indicating an enrichment of these cell types. Isolated MSCs from SCD patients with pre-collapse ONFH maintained the replicative capacity without significant loss of their specific biomolecular characteristics, multi-differentiation potential, and osteogenic differentiation activities. Cytokines and growth factors (interleukin-8, transforming growth factor-beta, stromal cell-derived factor-1alpha and vascular endothelial growth factor) that mediate endogenous bone regeneration were also produced by expanded MSCs from SCD patients.
Conclusion: The autologous BMMC implantation with a minimally invasive technique resulted in significant pain relief and halted the progression of early stages of ONFH in SCD patients. MSCs from SCD patients display biological properties that may add to the efficiency of surgical treatment in ONFH. In summary, our results indicate that infusion of BMMCs enriched with stem/progenitor cells is a safe and effective treatment for the early stages of ONFH in SCD patients.
Trial registration: ClinicalTrials.gov NCT02448121; registered 15 May 2015.
Figures



References
-
- Adorno EV, Zanette A, Lyra I, Seixas MO, Reis MG, Gonçalves MS. Clinical and molecular characteristics of sickle cell anemia in the northeast of Brazil. Genet Mol Biol. 2008;31:621–5. doi: 10.1590/S1415-47572008000400003. - DOI
-
- Acurio MT, Friedman RJ. Hip arthroplasty in patients with sickle-cell haemoglobinopathy. J Bone Joint Surg (Br) 1992;74:367–71. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
