

Directly observed therapy for treating tuberculosis
- PMID: 26022367
- PMCID: PMC4460720
- DOI: 10.1002/14651858.CD003343.pub4
Directly observed therapy for treating tuberculosis
Abstract
Background: Tuberculosis (TB) requires at least six months of treatment. If treatment is incomplete, patients may not be cured and drug resistance may develop. Directly Observed Therapy (DOT) is a specific strategy, endorsed by the World Health Organization, to improve adherence by requiring health workers, community volunteers or family members to observe and record patients taking each dose.
Objectives: To evaluate DOT compared to self-administered therapy in people on treatment for active TB or on prophylaxis to prevent active disease. We also compared the effects of different forms of DOT.
Search methods: We searched the following databases up to 13 January 2015: the Cochrane Infectious Diseases Group Specialized Register; the Cochrane Central Register of Controlled Trials (CENTRAL), published in the Cochrane Library; MEDLINE; EMBASE; LILACS and mRCT. We also checked article reference lists and contacted relevant researchers and organizations.
Selection criteria: Randomized controlled trials (RCTs) and quasi-RCTs comparing DOT with routine self-administration of treatment or prophylaxis at home.
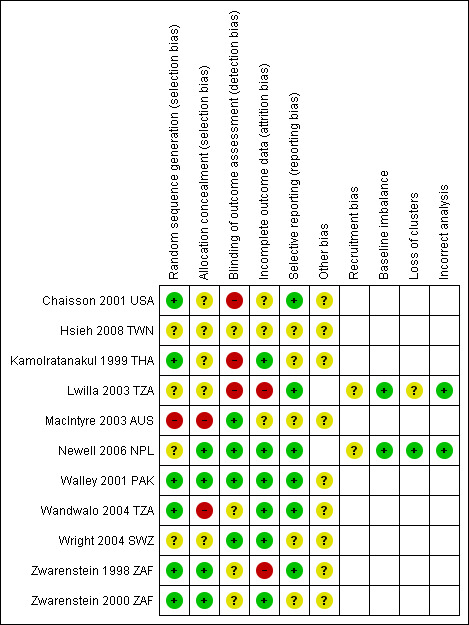
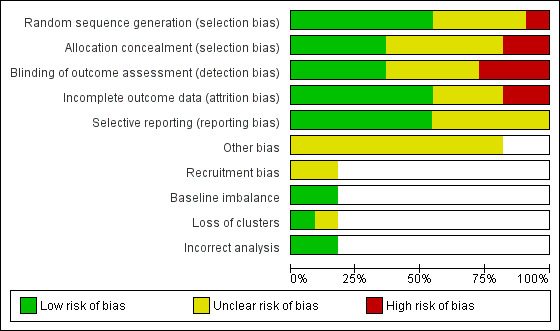
Data collection and analysis: Two review authors independently assessed risk of bias of each included trial and extracted data. We compared interventions using risk ratios (RR) with 95% confidence intervals (CI). We used a random-effects model if meta-analysis was appropriate but heterogeneity present (I(2) statistic > 50%). We assessed the quality of the evidence using the GRADE approach.
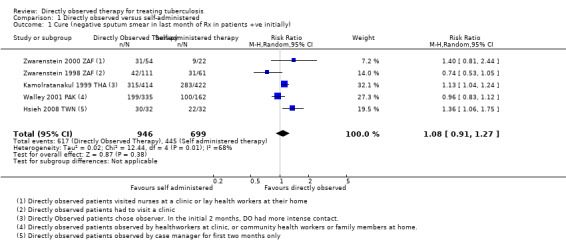
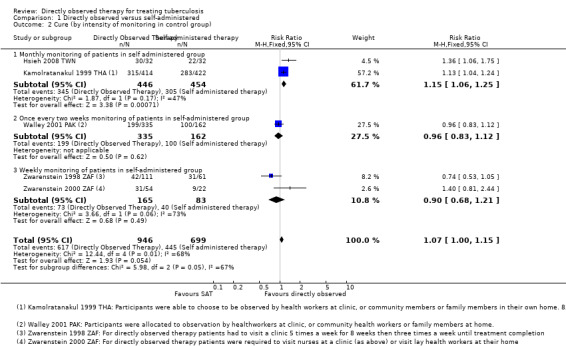
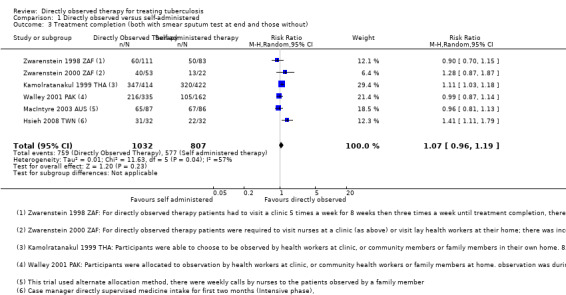
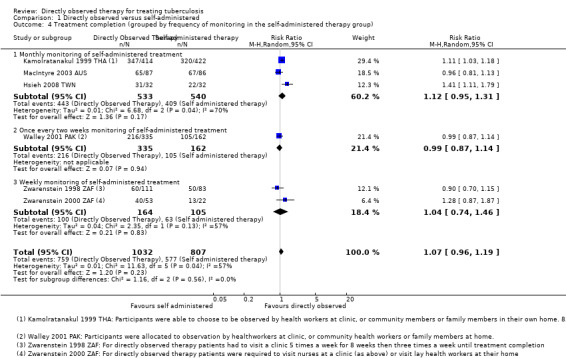
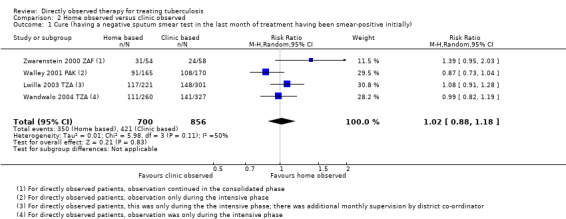
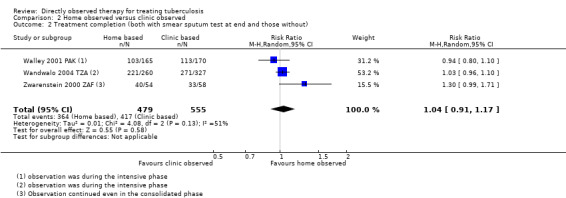
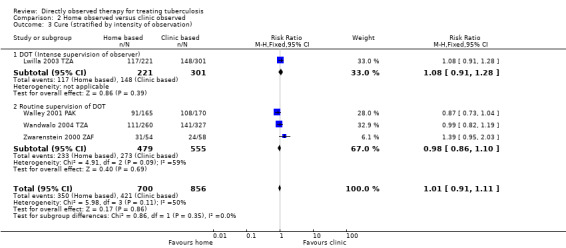
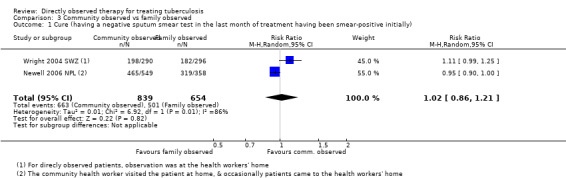
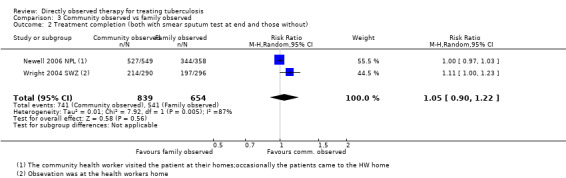
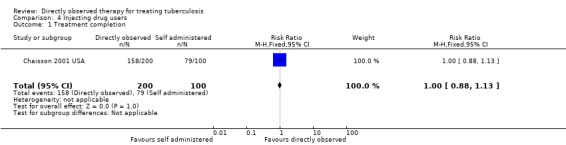
Main results: Eleven trials including 5662 participants met the inclusion criteria. DOT was performed by a range of people (nurses, community health workers, family members or former TB patients) in a variety of settings (clinic, the patient's home or the home of a community volunteer). DOT versus self-administered Six trials from South Africa, Thailand, Taiwan, Pakistan and Australia compared DOT with self-administered therapy for treatment. Trials included DOT at home by family members, community health workers (who were usually supervised); DOT at home by health staff; and DOT at health facilities. TB cure was low with self-administration across all studies (range 41% to 67%), and direct observation did not substantially improve this (RR 1.08, 95% CI 0.91 to 1.27; five trials, 1645 participants, moderate quality evidence). In a subgroup analysis stratified by the frequency of contact between health services in the self-treatment arm, daily DOT may improve TB cure when compared to self-administered treatment where patients in the self-administered group only visited the clinic every month (RR 1.15, 95% CI 1.06 to 1.25; two trials, 900 participants); but with contact in the control becoming more frequent, this small effect was not apparent (every two weeks: RR 0.96, 95% CI 0.83 to 1.12; one trial, 497 participants; every week: RR 0.90, 95% CI 0.68 to 1.21; two trials, 248 participants).Treatment completion showed a similar pattern, ranging from 59% to 78% in the self-treatment groups, and direct observation did not improve this (RR 1.07, 95% CI 0.96 to 1.19; six trials, 1839 participants, moderate quality evidence). DOT at home versus DOT at health facility In four trials that compared DOT at home by family members, or community health workers, with DOT by health workers at a health facility there was little or no difference in cure or treatment completion (cure: RR 1.02, 95% CI 0.88 to 1.18, four trials, 1556 participants, moderate quality evidence; treatment completion: RR 1.04, 95% CI 0.91 to 1.17, three trials, 1029 participants, moderate quality evidence). DOT by family member versus DOT by community health workerTwo trials compared DOT at home by family members with DOT at home by community health workers. There was also little or no difference in cure or treatment completion (cure: RR 1.02, 95% CI 0.86 to 1.21; two trials, 1493 participants, moderate quality evidence; completion: RR 1.05, 95% CI 0.90 to 1.22; two trials, 1493 participants, low quality evidence). Specific patient categoriesA trial of 300 intravenous drug users in the USA evaluated direct observation with no observation in TB prophylaxis to prevent active disease and showed little difference in treatment completion (RR 1.00, 95% CI 0.88 to 1.13; one trial, 300 participants, low quality evidence).
Authors' conclusions: From the existing trials, DOT did not provide a solution to poor adherence in TB treatment. Given the large resource and cost implications of DOT, policy makers might want to reconsider strategies that depend on direct observation. Other options might take into account financial and logistical barriers to care; approaches that motivate patients and staff; and defaulter follow-up.
Conflict of interest statement
As a result of the earlier editions of this review from the mid 1990s, PG has become recognised and associated with the continued debate about whether DOT should be central to national programmes in low‐ and middle‐income countries.
Figures
Update of
-
Directly observed therapy for treating tuberculosis.Cochrane Database Syst Rev. 2007 Oct 17;(4):CD003343. doi: 10.1002/14651858.CD003343.pub3. Cochrane Database Syst Rev. 2007. Update in: Cochrane Database Syst Rev. 2015 May 29;(5):CD003343. doi: 10.1002/14651858.CD003343.pub4. PMID: 17943789 Updated.
Comment in
-
Directly observed treatment is not the only solution for poor adherence and low cure of tuberculosis.Evid Based Med. 2015 Oct;20(5):180. doi: 10.1136/ebmed-2015-110247. Epub 2015 Aug 20. Evid Based Med. 2015. PMID: 26294788 No abstract available.
References
References to studies included in this review
Chaisson 2001 USA {published data only}
-
- Chaisson RE, Barnes GL, Hackman J, Watkinson L, Kimbrough L, Metha S, et al. A randomized, controlled trial of interventions to improve adherence to isoniazid therapy to prevent tuberculosis in injection drug users. American Journal of Medicine 2001;110(8):610‐5. - PubMed
Hsieh 2008 TWN {published data only}
-
- Hsieh CJ, Lin LC, Kuo BI, Chiang CH, Su WJ, Shih JF. Exploring the efficacy of a case management model using DOTS in the adherence of patients with pulmonary tuberculosis. Journal of Clinical Nursing 2008;17(7):869‐75. - PubMed
Kamolratanakul 1999 THA {published data only}
-
- Kamolratanakul P, Sawert H, Lertmaharit S, Kasetjaroen Y, Akksilp S, Tulaporn C, et al. Randomized controlled trial of directly observed treatment (DOT) for patients with pulmonary tuberculosis in Thailand. Transactions of the Royal Society of Tropical Medicine and Hygiene 1999;93(5):552‐7. - PubMed
Lwilla 2003 TZA {published data only}
-
- Lwilla F, Schellenberg D, Masanja H, Acosta C, Galindo C, Aponte J, et al. Evaluation of efficacy of community‐based vs. institutional‐based direct observed short‐course treatment for the control of tuberculosis in Kilombero district, Tanzania. Tropical Medicine and International Health 2003;8(3):204‐10. - PubMed
MacIntyre 2003 AUS {published data only}
-
- MacIntyre CR, Goebel K, Brown GV, Skull S, Starr M, Fullinfaw RO. A randomised controlled trial of the efficacy of family‐based direct observation of anti‐tuberculosis treatment in an urban, developed‐country setting. International Journal of Tuberculosis and Lung Disease 2003;7(9):848‐54. - PubMed
Newell 2006 NPL {published data only}
-
- Newell JN, Baral SC, Pande SB, Bam DS, Malla P. Family‐member DOTS and community DOTS for tuberculosis control in Nepal: cluster‐randomised controlled trial. Lancet 2006;367(9514):903‐9. - PubMed
Walley 2001 PAK {published data only}
-
- Khan MA, Walley JD, Witter SN, Imran A, Safdar N. Costs and cost‐effectiveness of different DOT strategies for the treatment of tuberculosis in Pakistan. Directly Observed Treatment. Health Policy and Planning 2002;17(2):178‐86. - PubMed
-
- Walley JD, Khan MA, Newell JN, Khan MH. Effectiveness of direct observation component of DOTS for tuberculosis: a randomised controlled trial in Pakistan. Lancet 2001;357(9275):664‐9. - PubMed
Wandwalo 2004 TZA {published data only}
-
- Wandwalo E, Kapalata N, Egwaga S, Morkve O. Effectiveness of community‐based directly observed treatment for tuberculosis in an urban setting in Tanzania: a randomised controlled trial. International Journal of Tuberculosis and Lung Disease 2004;8(10):1248‐54. - PubMed
Wright 2004 SWZ {published data only}
-
- Wright J, Walley J, Phillip A, Pushpananthan S, Dlamini E, Newell J, et al. Direct observation of treatment for tuberculosis: a randomized controlled trial of community health workers versus family members. Tropical Medicine and International Health 2004;9(5):559‐65. - PubMed
Zwarenstein 1998 ZAF {published data only}
-
- Zwarenstein M, Schoeman JH, Vundule C, Lombard CJ, Tatley M. Randomised controlled trial of self‐supervised and directly observed treatment of tuberculosis. Lancet 1998;352(9137):1340‐3. - PubMed
Zwarenstein 2000 ZAF {published data only}
-
- Zwarenstein M, Schoeman JH, Vundule C, Lombard CJ, Tatley M. A randomised trial of lay health workers as direct observers for treatment of tuberculosis. International Journal of Tuberculosis and Lung Disease 2000;4(6):550‐4. - PubMed
References to studies excluded from this review
Batki 2002 {published data only}
-
- Batki SL, Gruber VA, Bradley JM, Bradley M, Delucchi K. A controlled trial of methadone treatment combined with directly observed isoniazid for tuberculosis prevention in injection drug users. Drug and Alcohol Dependence 2002;66(3):283‐93. - PubMed
Carroll 2004 {published data only}
-
- Carroll K, Malefoasi G. Comparison of outcomes from a district tuberculosis control programme in the Pacific: before and after the implementation of DOTS. Tropical Doctor 2004;34(1):11‐4. - PubMed
Hwang 2004 {published data only}
-
- Hwang TG, Kim SD, Yoo SH, Shin YC. Sputum smear conversion during mDOT. Tuberculosis and Respiratory Diseases 2004;56(5):485‐94.
Jasmer 2004 {published data only}
-
- Jasmer RM, Seaman CB, Gonzalez LC, Kawamura LM, Osmond DH, Daley CL. Tuberculosis treatment outcomes: directly observed therapy compared with self‐administered therapy. American Journal of Respiratory and Critical Care Medicine 2004;170(5):561‐6. - PubMed
Lewin 2004 {published data only}
Malotte 2001 {published data only}
-
- Malotte CK, Hollingshead JR, Larro M. Incentives vs outreach workers for latent tuberculosis treatment in drug users. American Journal of Preventive Medicine 2001;20(2):103‐7. - PubMed
Matthew 2002 {published data only}
-
- Matthew AJ, Eicher A, Davies PD. Comparison of hospital checked directly observed therapy with family supervised and unchecked tuberculosis treatment in a rural setting in North India. European Respiratory Journal 2002;20(Suppl 38):215.
Moulding 2002 {published data only}
-
- Moulding TS, Caymittes M. Managing medication compliance of tuberculosis patients in Haiti with medication monitors. International Journal of Tuberculosis and Lung Disease 2002;6(4):313‐9. - PubMed
Pungrassami 2002a {published data only}
-
- Pungrassami P, Johnsen SP, Chongsuvivatwong V, Olsen J. Has directly observed treatment improved outcomes for patients with tuberculosis in southern Thailand?. Tropical Medicine and International Health 2002;7(3):271‐9. - PubMed
Pungrassami 2002b {published data only}
-
- Pungrassami P, Chongsuvivatwong V. Are health personnel the best choice for directly observed treatment in southern Thailand? A comparison of treatment outcomes among different types of observers. Transactions of the Royal Society of Tropical Medicine and Hygiene 2002;96(6):695‐9. - PubMed
Sorete‐Abore 2002 {published data only}
-
- Sorete‐Arbore A, Mihaescu T. Three years of DOTS strategy in Iasi county, Romania. European Respiratory Journal 2002;20(Suppl 38):217.
Tandon 2002 {published data only}
-
- Tandon M, Gupta M, Tandon S, Gupta KB. DOTS versus self administered therapy (SAT) for patients with pulmonary tuberculosis: a randomised trial at a tertiary care hospital. Indian Journal of Medical Science 2002;56(1):19‐21. - PubMed
Thiam 2007 {published data only}
-
- Thiam S, LeFevre AM, Hane F, Ndiaye A, Ba F, Fielding KL, et al. Effectiveness of a strategy to improve adherence to tuberculosis treatment in a resource‐poor setting: a cluster randomized controlled trial. JAMA 2007;297(4):380‐6. - PubMed
Toyota 2003 {published data only}
-
- Toyota E, Kobayashi N, Houjou M, Yoshizawa A, Kawana A, Kudo K. Usefulness of directly observed therapy (DOT) during hospitalization as DOTS in Japanese style. Kekkaku 2003;78(9):581‐5. - PubMed
Additional references
Anuwatnonthakate 2008
Barbara 2013
-
- Seaworth BJ, Armitige LY, Griffith DE. First do no harm—adverse events, drug intolerance, and hepatotoxicity: how can we not justify directly observed therapy for treating tuberculosis?. Clinical Infectious Diseases 2013;57(7):1063‐4. - PubMed
Bayer 1995
-
- Bayer R, Wilkinson D. Directly observed therapy for tuberculosis: history of an idea. Lancet 1995;345(8964):1545‐8. - PubMed
Bosch‐Capblanch 2007
-
- Bosch‐Capblanch X, Abba K, Prictor M, Garner P. Contracts between patients and healthcare practitioners for improving patients' adherence to treatment, prevention and health promotion activities. Cochrane Database of Systematic Reviews 2007, Issue 2. [DOI: 10.1002/14651858.CD004808.pub3] - DOI - PMC - PubMed
Chan 2002
Chaulk 1998
-
- Chaulk CP, Kazandjian VA. Directly observed therapy for treatment completion of pulmonary tuberculosis: Consensus Statement of the Public Health Tuberculosis Guidelines Panel. JAMA 1998;279(12):943‐8. - PubMed
Chien 2013
-
- Chien JY, Lai CC, Tan CK, Chien ST, Yu CJ, Hsueh PR. Decline in rates of acquired multidrug‐resistant tuberculosis after implementation of the directly observed therapy, short course (DOTS) and DOTS‐Plus programmes in Taiwan. Journal of Antimicrobial Chemotherapy 2013;68(8):1910–6. - PubMed
Dick 2005
-
- Dick J, Murray E, Botha E. Operations Research Results. The effectiveness of TB DOTS supporters in South Africa. April 2005. https://www.usaidassist.org/sites/assist/files/pnadf972.pdf (accessed 23 January 2014).
Ford 2009
-
- Ford N, Nachega JB, Engel ME, Mills EJ. Directly observed antiretroviral therapy: a systematic review and meta‐analysis of randomised clinical trials. Lancet 2009;374(9707):2064‐71. - PubMed
Frieden 2003
-
- Frieden TR, Sterling TR, Munsiff SS, Watt CJ, Dye C. Tuberculosis. Lancet 2003;362(9387):887‐99. - PubMed
Frieden 2007
Gross 2009
Higgins 2011
-
- Higgins J, Green S (editors). Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org (accessed 20 August 2013).
Hirpa 2013
Hopewell 2006
-
- Hopewell PC, Pai M, Maher D, Uplekar M, Raviglione MC. International Standards for Tuberculosis Care. Lancet Infectious Diseases 2006;6(11):710‐25. - PubMed
Jüni 2001
Khan 2003
-
- Khan MA, Walley JD, Witter SN, Imran A, Safdar N. Cost and cost effectiveness of different DOT strategies for the treatment of tuberculosis in Pakistan. Directly observed treatment. Health Policy and Planning 2003;17(2):178‐86. - PubMed
Liu 2008
Lutge 2012
M'Imunya 2012
Macq 2003
-
- Macq JC, Theobald S, Dick J, Dembele M. An exploration of the concept of directly observed treatment (DOT) for tuberculosis patients: from a uniform to a customised approach. International Journal of Tuberculosis and Lung Disease 2003;7(2):103‐9. - PubMed
Mohan 2007
-
- Mohan CI, Bishai D, Cavalcante S, Chaisson RE. The cost‐effectiveness of DOTS in urban Brazil. International Journal of Tuberculosis and Lung Disease 2007;11(1):27‐32. - PubMed
Moonan 2011
Munro 2007
Pasipanodya 2013
Review Manager 5 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Sepkowitz 1995
Smieja 2010
Steffen 2010
Tian 2014
van den Boogaard 2012
-
- Boogaard J, Msoka E, Homfray M, Kibiki GS, Heldens JJ, Felling AJ, et al. An exploration of patients perceptions of adherence to tuberculosis treatment in Tanzania. Qualitative Health Research 2012;22(6):835‐45. - PubMed
Volmink 2000b
-
- Volmink J, Matchaba P, Garner P. Directly observed therapy and treatment adherence. Lancet 2000;355(9212):1345‐50. - PubMed
WHO 2002
-
- WHO Global Tuberculosis Programme. An Expanded DOTS Framework for Effective Tuberculosis Control. Stop TB Communicable Diseases. Geneva: World Health Organization, 2002.
WHO 2010
-
- World Health Organization. Treatment of tuberculosis guidelines: Fourth edition. 2010. http://apps.who.int/iris/bitstream/10665/44165/1/9789241547833_eng.pdf?u... (accessed 01 August 2014).
WHO 2013
-
- WHO Global TB Programme. Global Tuberculosis Report 2013. http://apps.who.int/iris/bitstream/10665/91355/1/9789241564656_eng.pdf (accessed 01 August 2014).
References to other published versions of this review
Volmink 1997
Volmink 2000a
Volmink 2001
-
- Volmink J, Garner P. Directly observed therapy for treating tuberculosis. Cochrane Database of Systematic Reviews 2001, Issue 4. [DOI: 10.1002/14651858.CD003343] - PubMed
Volmink 2003
Volmink 2006
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous