

Additive beneficial effects of valsartan combined with rosuvastatin in the treatment of hypercholesterolemic hypertensive patients
- PMID: 26023311
- PMCID: PMC4446817
- DOI: 10.4070/kcj.2015.45.3.225
Additive beneficial effects of valsartan combined with rosuvastatin in the treatment of hypercholesterolemic hypertensive patients
Erratum in
-
Erratum to: Additive Beneficial Effects of Valsartan Combined with Rosuvastatin in the Treatment of Hypercholesterolemic Hypertensive Patients.Korean Circ J. 2015 Jul;45(4):349. doi: 10.4070/kcj.2015.45.4.349. Korean Circ J. 2015. PMID: 26240593 Free PMC article.
Abstract
Background and objectives: We compared the efficacy and safety of valsartan and rosuvastatin combination therapy with each treatment alone in hypercholesterolemic hypertensive patients.
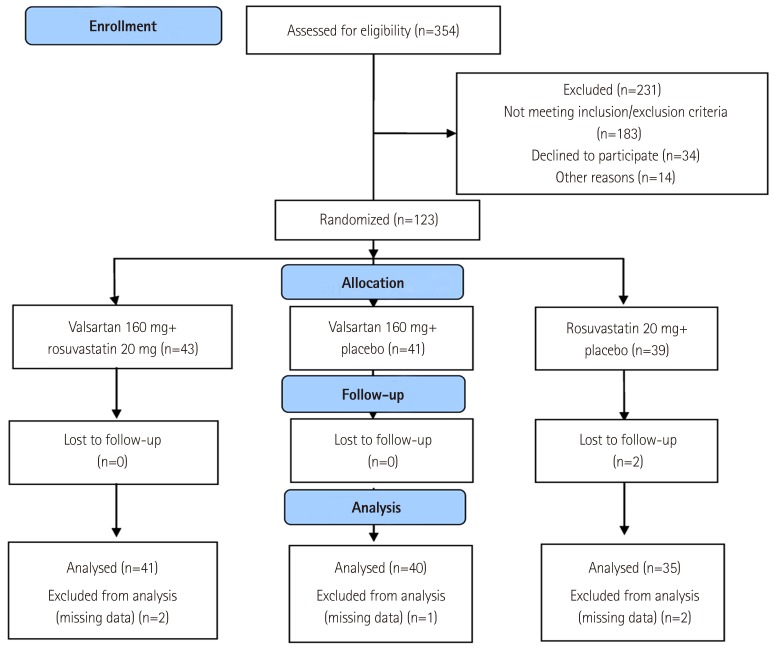
Subjects and methods: Patients who met inclusion criteria were randomized to receive 1 of the following 2-month drug regimens: valsartan 160 mg plus rosuvastatin 20 mg, valsartan 160 mg plus placebo, or rosuvastatin 20 mg plus placebo. The primary efficacy variables were change in sitting diastolic blood pressure (sitDBP) and sitting systolic blood pressure (sitSBP), and percentage change in low-density lipoprotein-cholesterol (LDL-C) in the combination, valsartan, and rosuvastatin groups. Adverse events (AEs) during the study were analyzed.
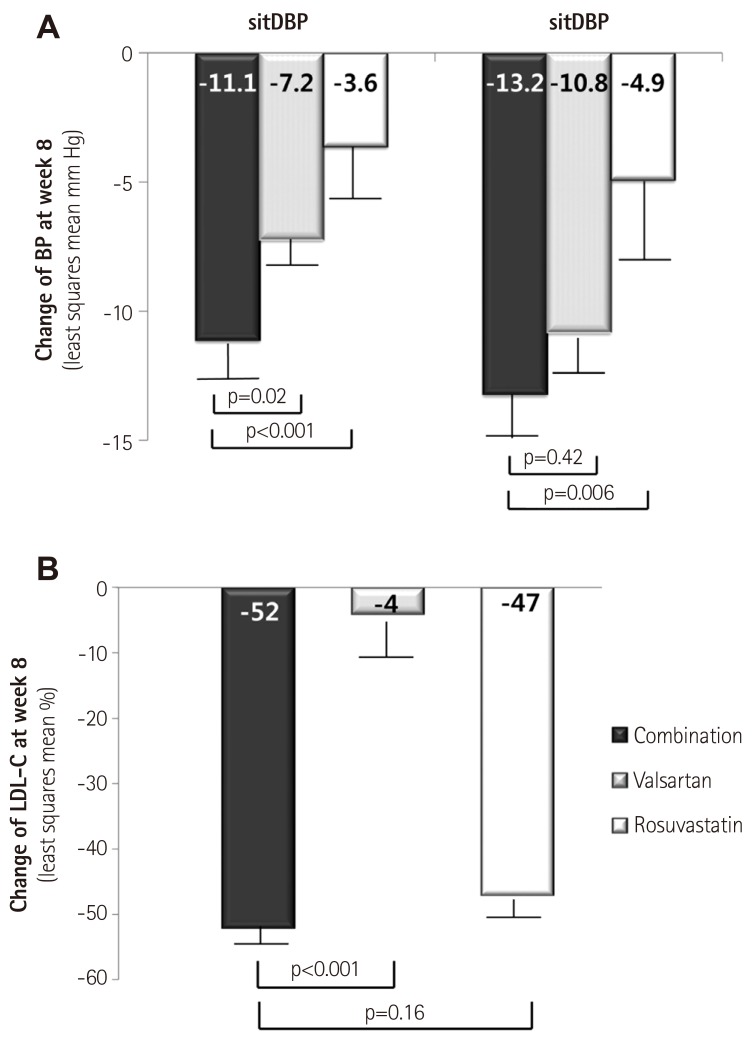
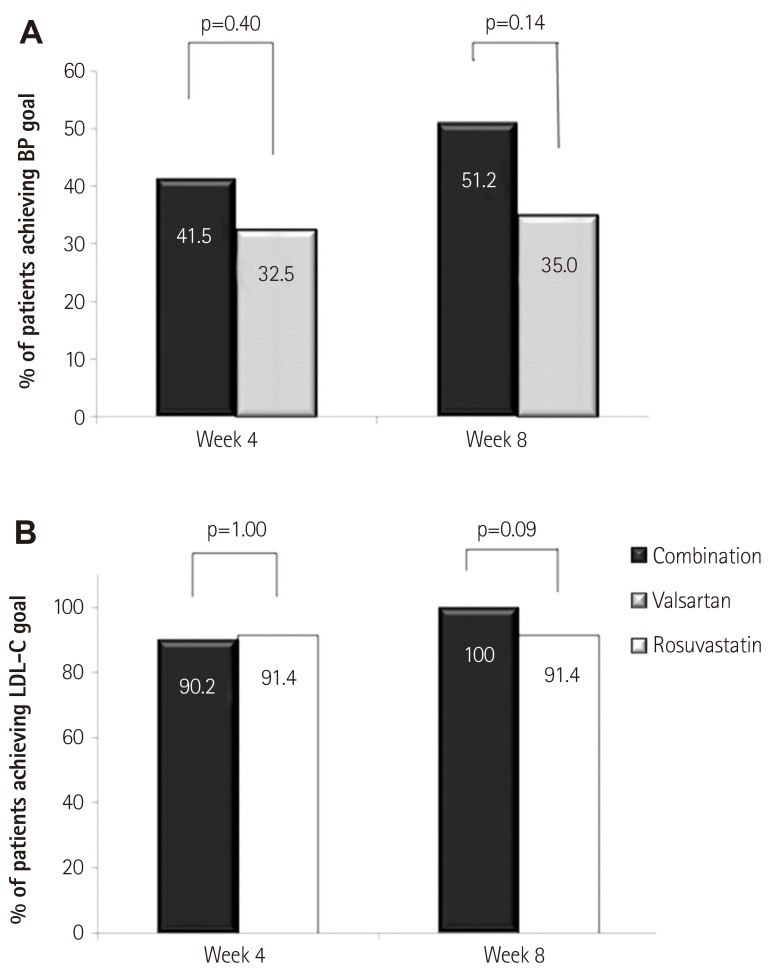
Results: A total of 354 patients were screened and 123 of them were finally randomized. Changes of sitDBP by least squares mean (LSM) were -11.1, -7.2, and -3.6 mm Hg, respectively, and was greater in the combination, as compared to both valsartan (p=0.02) and rosuvastatin (p<0.001). Changes of sitSBP by LSM were -13.2, -10.8, and -4.9 mm Hg, and was greater in the combination, as compared to rosuvastatin (p=0.006) and not valsartan (p=0.42). Percentage changes of LDL-C by LSM were -52, -4, and -47% in each group, and was greater in the combination, as compared to valsartan (p<0.001), similar to rosuvastatin (p=0.16). Most AEs were mild and resolved by the end of the study.
Conclusion: Combination treatment with valsartan and rosuvastatin exhibited an additive blood pressure-lowering effect with acceptable tolerability, as compared to valsartan monotherapy. Its lipid lowering effect was similar to rosuvatatin monotherapy.
Keywords: Blood pressure; Controlled clinical trials, randomized; Drug therapy, combination; Rosuvastatin; Valsartan.
Figures
References
-
- Kannel WB. Blood pressure as a cardiovascular risk factor: prevention and treatment. JAMA. 1996;275:1571–1576. - PubMed
-
- Thomas F, Bean K, Guize L, Quentzel S, Argyriadis P, Benetos A. Combined effects of systolic blood pressure and serum cholesterol on cardiovascular mortality in young (<55 years) men and women. Eur Heart J. 2002;23:528–535. - PubMed
-
- James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8) JAMA. 2014;311:507–520. - PubMed
-
- Nickenig G, Harrison DG. The AT(1)-type angiotensin receptor in oxidative stress and atherogenesis: Part II: AT(1) receptor regulation. Circulation. 2002;105:530–536. - PubMed
-
- Keidar S, Kaplan M, Shapira C, Brook JG, Aviram M. Low density lipoprotein isolated from patients with essential hypertension exhibits increased propensity for oxidation and enhanced uptake by macrophages: a possible role for angiotensin II. Atherosclerosis. 1994;107:71–84. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
