

Living with, managing and minimising treatment burden in long term conditions: a systematic review of qualitative research
- PMID: 26024379
- PMCID: PMC4449201
- DOI: 10.1371/journal.pone.0125457
Living with, managing and minimising treatment burden in long term conditions: a systematic review of qualitative research
Abstract
Background: 'Treatment burden', defined as both the workload and impact of treatment regimens on function and well-being, has been associated with poor adherence and unfavourable outcomes. Previous research focused on treatment workload but our understanding of treatment impact is limited. This research aimed to systematically review qualitative research to identify: 1) what are the treatment generated disruptions experienced by patients across all chronic conditions and treatments? 2) what strategies do patients employ to minimise these treatment generated disruptions?
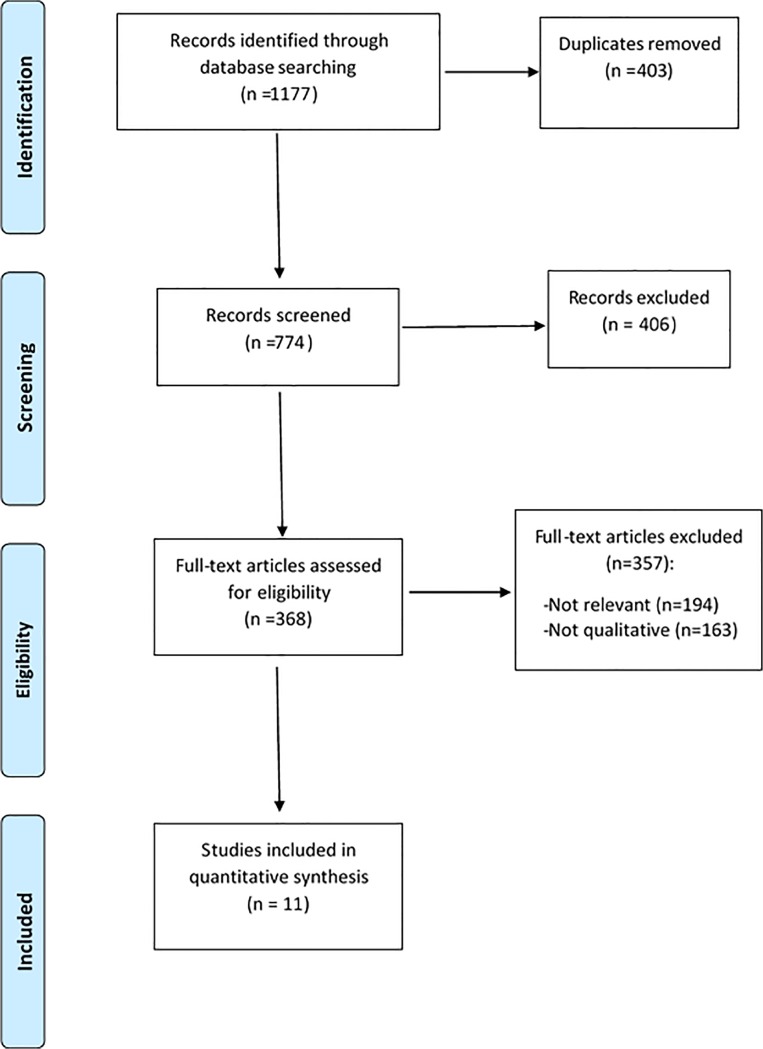
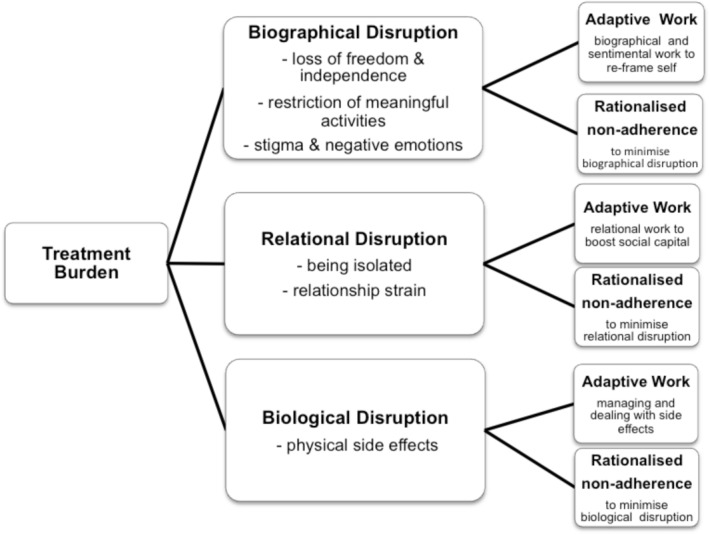
Methods and findings: The search strategy centred on: treatment burden and qualitative methods. Medline, CINAHL, Embase, and PsychINFO were searched electronically from inception to Dec 2013. No language limitations were set. Teams of two reviewers independently conducted paper screening, data extraction, and data analysis. Data were analysed using framework synthesis informed by Cumulative Complexity Model. Eleven papers reporting data from 294 patients, across a range of conditions, age groups and nationalities were included. Treatment burdens were experienced as a series of disruptions: biographical disruptions involved loss of freedom and independence, restriction of meaningful activities, negative emotions and stigma; relational disruptions included strained family and social relationships and feeling isolated; and, biological disruptions involved physical side-effects. Patients employed "adaptive treatment work" and "rationalised non-adherence" to minimise treatment disruptions. Rationalised non-adherence was sanctioned by health professionals at end of life; at other times it was a "secret-act" which generated feelings of guilt and impacted on family and clinical relationships.
Conclusions: Treatments generate negative emotions and physical side effects, strain relationships and affect identity. Patients minimise these disruptions through additional adaptive work and/or by non-adherence. This affects physical outcomes and care relationships. There is a need for clinicians to engage with patients in honest conversations about treatment disruptions and the 'adhere-ability' of recommended regimens. Patient-centred practice requires management plans which optimise outcomes and minimise disruptions.
Conflict of interest statement
Figures
References
-
- Corbin J, Strauss A. Managing chronic illness at home: Three lines of work. Qualitative Sociology. 1985;8(3):224–47.
-
- Bury M. The sociology of chronic illness: a review of research and prospects. Soctology of Health Si Illness. 1991;13(4):451–68.
-
- Janssens GO, Jansen MH, Lauwers SJ, Nowak PJ, Oldenburger FR, Bouffet E, et al. Hypofractionation vs conventional radiation therapy for newly diagnosed diffuse intrinsic pontine glioma: a matched-cohort analysis. International journal of radiation oncology, biology, physics. 2013;85(2):315–20. 10.1016/j.ijrobp.2012.04.006 - DOI - PubMed
-
- Grootscholten C, Ligtenberg G, Derksen RHWM, Schreurs KMG, de Glas-Vos JW, Hagen EC, et al. Health-related quality of life in patients with systemic lupus erythematosus: Development and validation of a lupus specific symptom checklist. Quality of Life Research. 2003;12:635–44. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
