

Clinical evaluation of an endorectal immobilization system for use in prostate hypofractionated Stereotactic Ablative Body Radiotherapy (SABR)
- PMID: 26024900
- PMCID: PMC4456701
- DOI: 10.1186/s13014-015-0426-4
Clinical evaluation of an endorectal immobilization system for use in prostate hypofractionated Stereotactic Ablative Body Radiotherapy (SABR)
Abstract
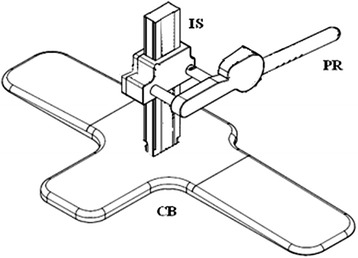
Background: The objective of this study was to evaluate a novel prostate endorectal immobilization system (EIS) for improving the delivery of hypofractionated Stereotactic Ablative Body Radiotherapy (SABR) for prostate cancer.
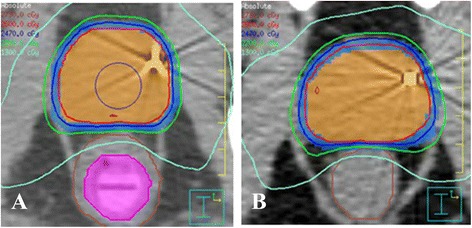
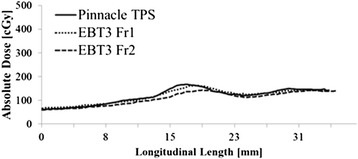
Methods: Twenty patients (n = 20) with low- or intermediate-risk prostate cancer (T1-T2b, Gleason Score < 7, PSA ≤ 20 ng/mL), were treated with an EIS in place using Volumetric Modulated Arc Therapy (VMAT), to a prescription dose of 26 Gy delivered in 2 fractions once per week; the intent of the institutional clinical trial was an attempt to replicate brachytherapy-like dosimetry using SABR. EBT3 radiochromic film embedded within the EIS was used as a quality assurance measure of the delivered dose; additionally, prostate intrafraction motion captured using pre- and post-treatment conebeam computed tomography (CBCT) scans was evaluated. Treatment plans were generated for patients with- and without the EIS to evaluate its effects on target and rectal dosimetry.
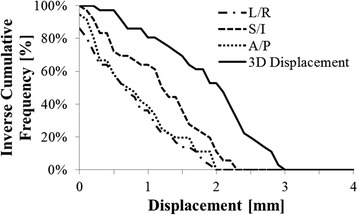
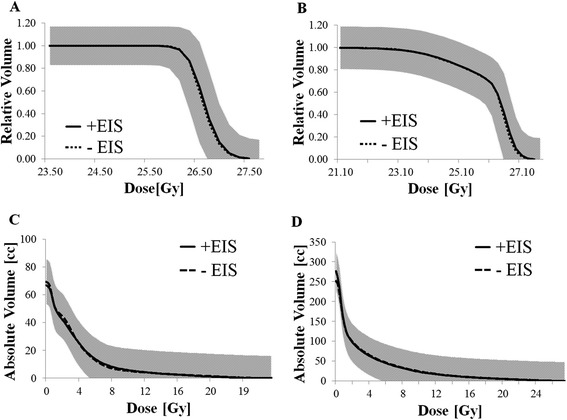
Results: None of the observed 3-dimensional prostate displacements were ≥ 3 mm over the elapsed treatment time. A Gamma passing rate of 95.64 ± 4.28 % was observed between planned and delivered dose profiles on EBT3 film analysis in the low-dose region. No statistically significant differences between treatment plans with- and without-EIS were observed for rectal, bladder, clinical target volume (CTV), and PTV contours (p = 0.477, 0.484, 0.487, and 0.487, respectively). A mean rectal V80% of 1.07 cc was achieved for plans using the EIS.
Conclusions: The EIS enables the safe delivery of brachytherapy-like SABR plans to the prostate while having minimal impact on treatment planning and rectal dosimetry. Consistent and reproducible immobilization of the prostate is possible throughout the duration of these treatments using such a device.
Figures
Similar articles
-
Dosimetric impact of organ at risk daily variation during prostate stereotactic ablative radiotherapy.Br J Radiol. 2020 Apr;93(1108):20190789. doi: 10.1259/bjr.20190789. Epub 2020 Jan 30. Br J Radiol. 2020. PMID: 31971829 Free PMC article.
-
Developing a class solution for Prostate Stereotactic Ablative Body Radiotherapy (SABR) using Volumetric Modulated Arc Therapy (VMAT).Radiother Oncol. 2014 Feb;110(2):298-302. doi: 10.1016/j.radonc.2013.10.036. Epub 2013 Dec 11. Radiother Oncol. 2014. PMID: 24332021 Free PMC article.
-
Efficacy of a rectal spacer with prostate SABR-first UK experience.Br J Radiol. 2018 Feb;91(1083):20170672. doi: 10.1259/bjr.20170672. Epub 2018 Jan 23. Br J Radiol. 2018. PMID: 29182384 Free PMC article.
-
Stereotactic body radiation therapy for prostate cancer-a review.Chin Clin Oncol. 2017 Sep;6(Suppl 2):S10. doi: 10.21037/cco.2017.06.05. Chin Clin Oncol. 2017. PMID: 28917248 Review.
-
Stereotactic Ablative Body Radiotherapy for Intermediate- or High-Risk Prostate Cancer.Cancer J. 2020 Jan/Feb;26(1):38-42. doi: 10.1097/PPO.0000000000000425. Cancer J. 2020. PMID: 31977383 Review.
Cited by
-
Urethra contouring on computed tomography urethrogram versus magnetic resonance imaging for stereotactic body radiotherapy in prostate cancer.Clin Transl Radiat Oncol. 2023 Dec 30;45:100722. doi: 10.1016/j.ctro.2023.100722. eCollection 2024 Mar. Clin Transl Radiat Oncol. 2023. PMID: 38234697 Free PMC article.
-
Stereotactic ablative body radiotherapy in patients with prostate cancer.Transl Androl Urol. 2018 Jun;7(3):330-340. doi: 10.21037/tau.2018.01.18. Transl Androl Urol. 2018. PMID: 30050794 Free PMC article. Review.
-
Effectiveness of rectal displacement devices in managing prostate motion: a systematic review.Strahlenther Onkol. 2021 Feb;197(2):97-115. doi: 10.1007/s00066-020-01633-9. Epub 2020 May 22. Strahlenther Onkol. 2021. PMID: 32444903
-
Comparison of VMAT-SABR treatment plans with flattening filter (FF) and flattening filter-free (FFF) beam for localized prostate cancer.J Appl Clin Med Phys. 2015 Nov 8;16(6):302–313. doi: 10.1120/jacmp.v16i6.5728. J Appl Clin Med Phys. 2015. PMID: 26699585 Free PMC article.
-
Rectal retractor in prostate radiotherapy: pros and cons.Radiat Oncol. 2022 Dec 9;17(1):204. doi: 10.1186/s13014-022-02176-2. Radiat Oncol. 2022. PMID: 36494732 Free PMC article.
References
-
- Miralbell R, Roberts SA, Zubizarreta E, Hendry JH. Dose-fractionation sensitivity of prostate cancer deduced from radiotherapy outcomes of 5,969 patients in seven international institutional datasets: α/β = 1.4 (0.9–2.2) Gy. Int J Radiat Oncol Biol Phys. 2012;82(1):e17–24. doi: 10.1016/j.ijrobp.2010.10.075. - DOI - PubMed
-
- Hodges BJC, Lotan Y, Boike TP, Benton R, Barrier A. Timmerman RD. Payer / Provider Relationships in Oncology Original Contributions, Cost-Effectiveness Analysis of Stereotactic Body Radiation Therapy Versus Intensity-Modulated Radiation Therapy: An Emerging Initial Radiation Treatment Option for Organ-Confined Prostate Cancer. J Oncol Pract. 2012;8(3 suppl):e31s–7. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
