

Change in coronary blood flow after percutaneous coronary intervention in relation to baseline lesion physiology: results of the JUSTIFY-PCI study
- PMID: 26025217
- PMCID: PMC4943523
- DOI: 10.1161/CIRCINTERVENTIONS.114.001715
Change in coronary blood flow after percutaneous coronary intervention in relation to baseline lesion physiology: results of the JUSTIFY-PCI study
Abstract
Background: Percutaneous coronary intervention (PCI) aims to increase coronary blood flow by relieving epicardial obstruction. However, no study has objectively confirmed this and assessed changes in flow over different phases of the cardiac cycle. We quantified the change in resting and hyperemic flow velocity after PCI in stenoses defined physiologically by fractional flow reserve and other parameters.
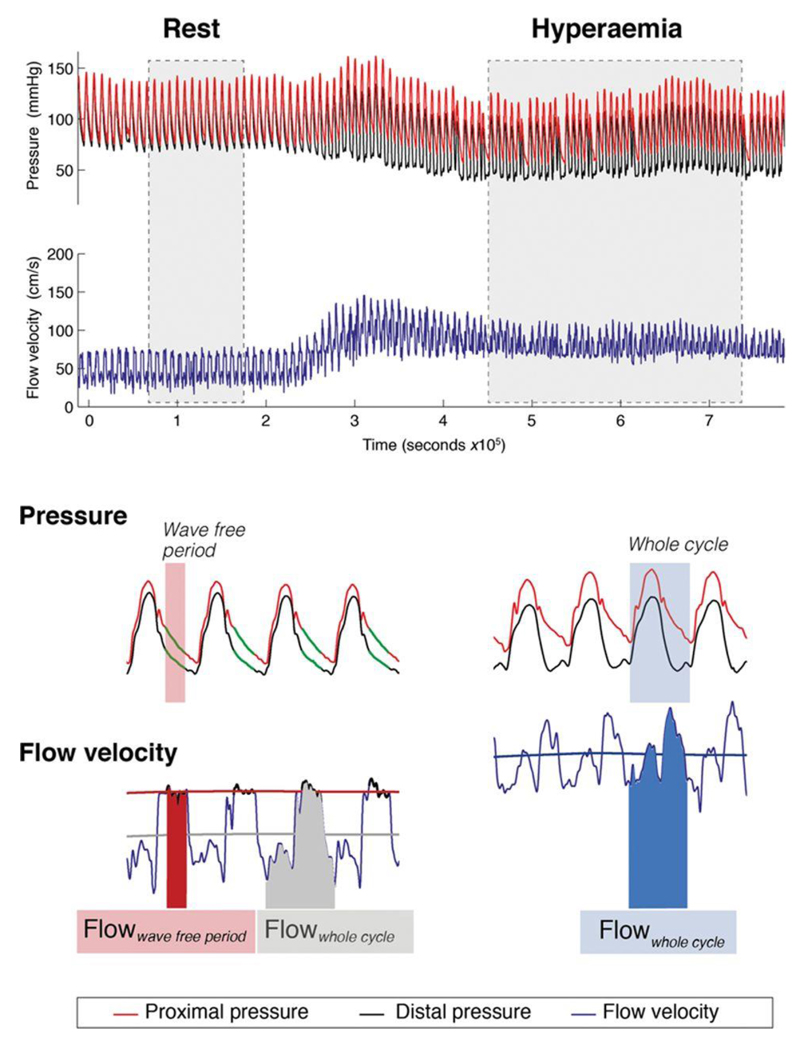
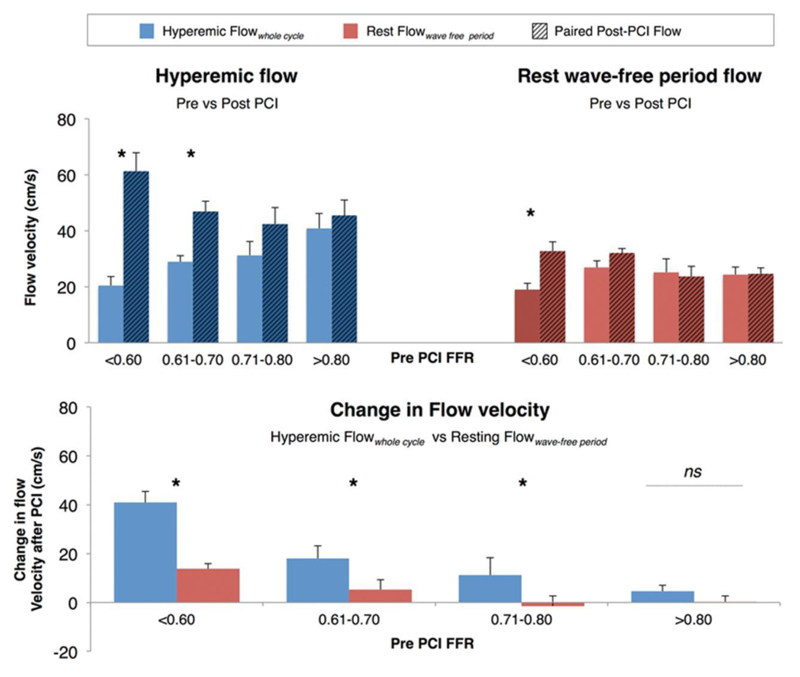
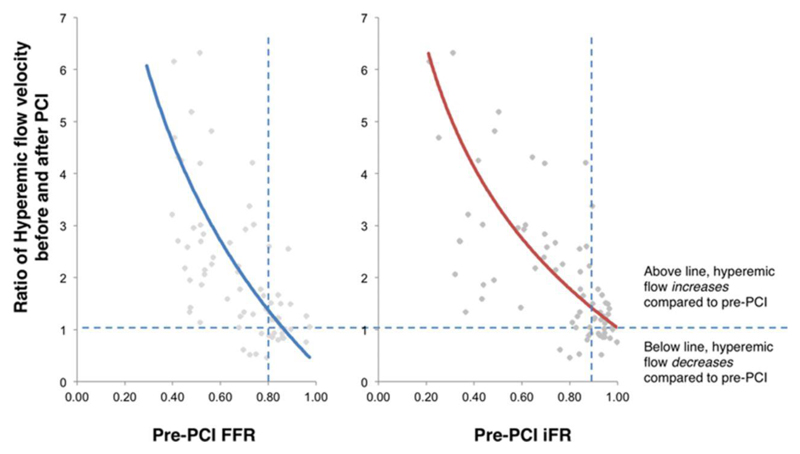
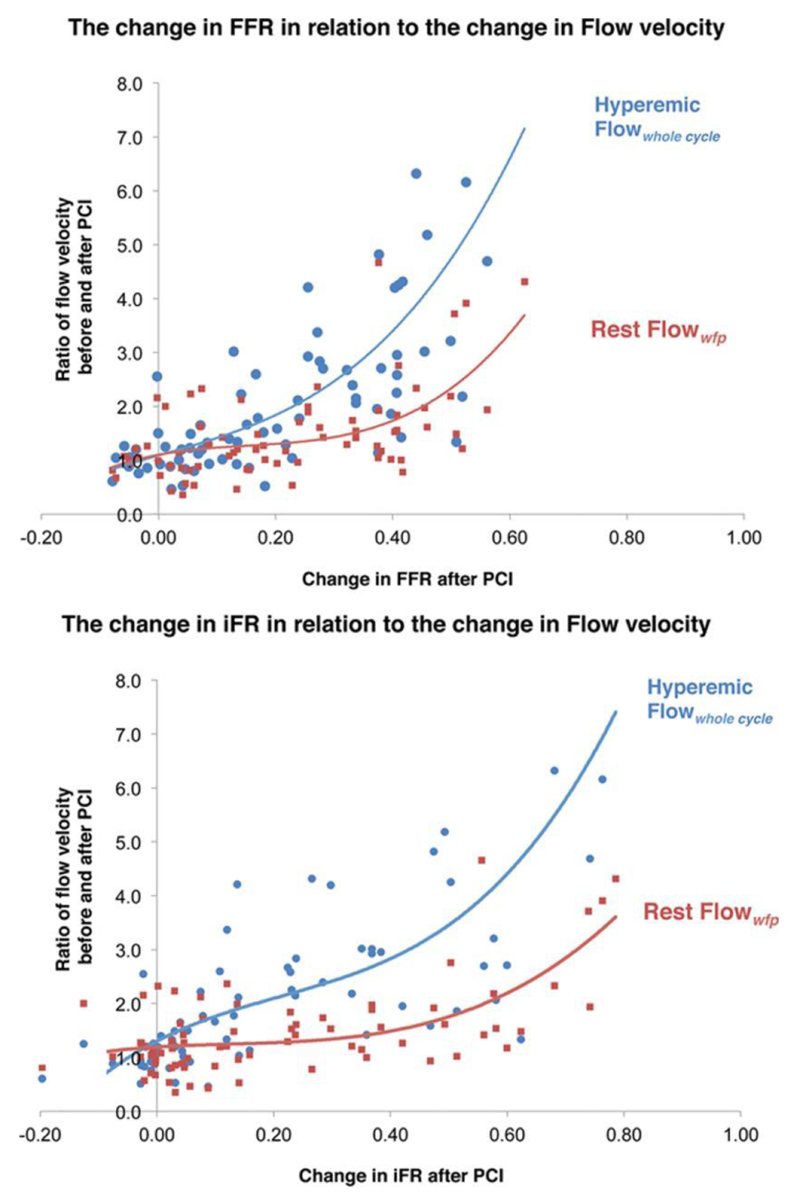
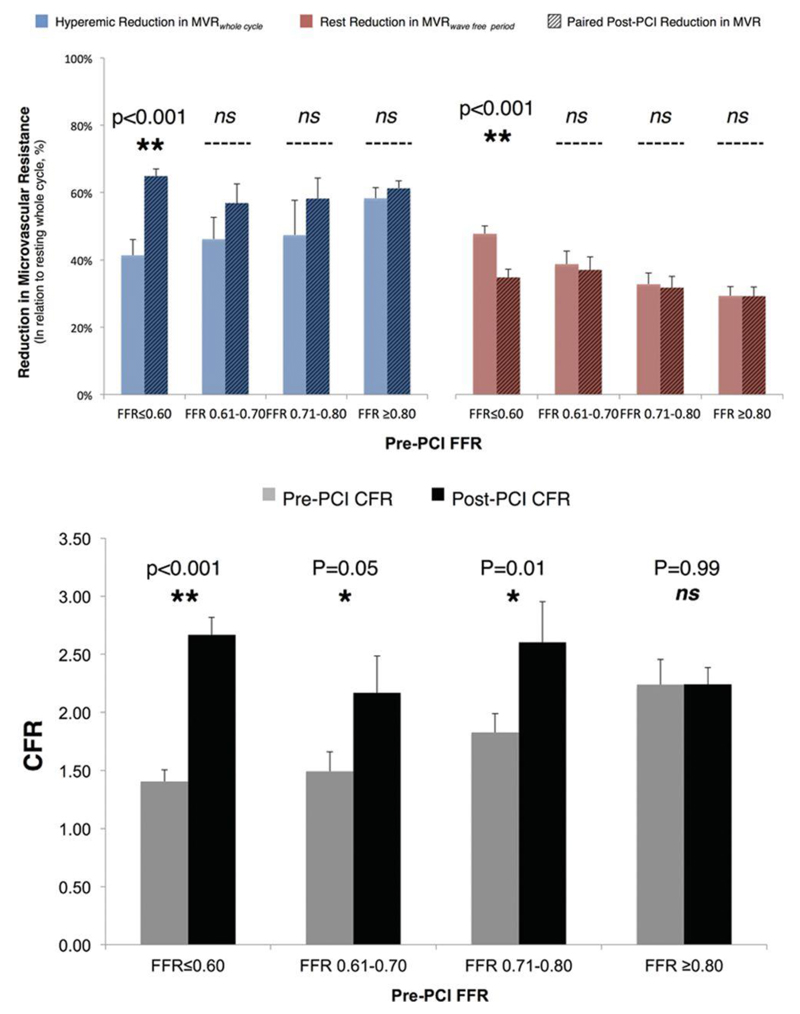
Methods and results: Seventy-five stenoses (67 patients) underwent paired flow velocity assessment before and after PCI. Flow velocity was measured over the whole cardiac cycle and the wave-free period. Mean fractional flow reserve was 0.68±0.02. Pre-PCI, hyperemic flow velocity is diminished in stenoses classed as physiologically significant compared with those classed nonsignificant (P<0.001). In significant stenoses, flow velocity over the resting wave-free period and hyperemic flow velocity did not differ statistically. After PCI, resting flow velocity over the wave-free period increased little (5.6±1.6 cm/s) and significantly less than hyperemic flow velocity (21.2±3 cm/s; P<0.01). The greatest increase in hyperemic flow velocity was observed when treating stenoses below physiological cut points; treating stenoses with fractional flow reserve ≤0.80 gained Δ28.5±3.8 cm/s, whereas those fractional flow reserve >0.80 had a significantly smaller gain (Δ4.6±2.3 cm/s; P<0.001). The change in pressure-only physiological indices demonstrated a curvilinear relationship to the change in hyperemic flow velocity but was flat for resting flow velocity.
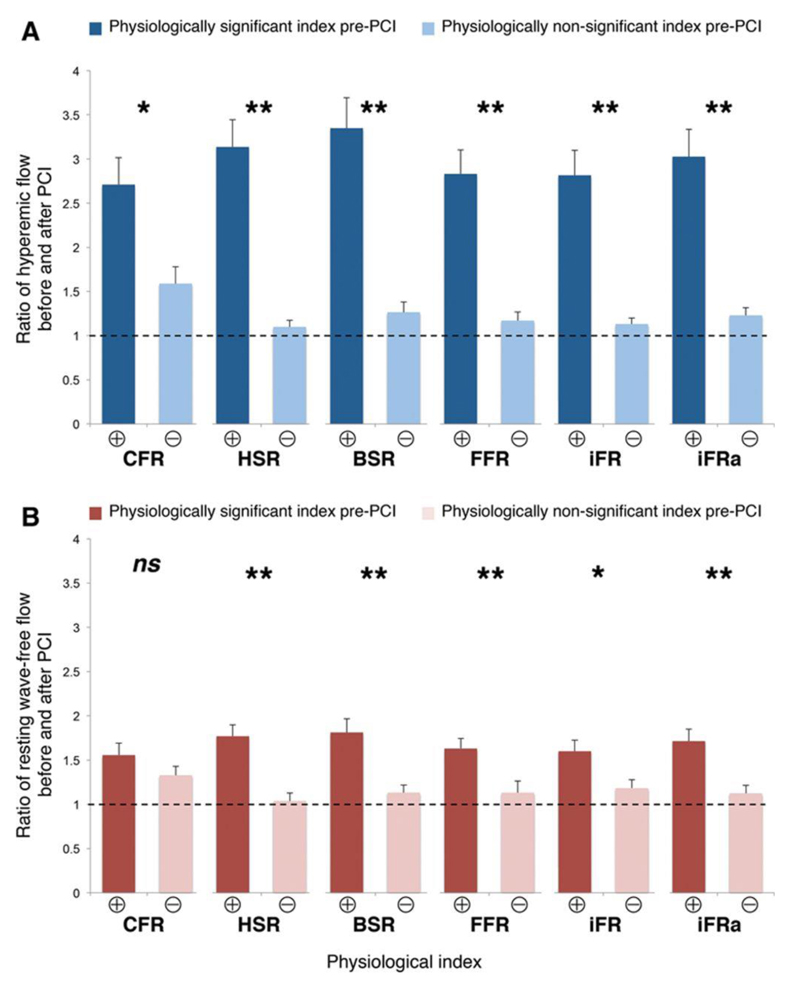
Conclusions: Pre-PCI physiology is strongly associated with post-PCI increase in hyperemic coronary flow velocity. Hyperemic flow velocity increases 6-fold more when stenoses classed as physiologically significant undergo PCI than when nonsignificant stenoses are treated. Resting flow velocity measured over the wave-free period changes at least 4-fold less than hyperemic flow velocity after PCI.
Keywords: angioplasty; blood flow velocity; percutaneous coronary intervention.
© 2015 American Heart Association, Inc.
Figures
References
-
- Boden WE, O’Rourke RA, Teo KK, Hartigan PM, Maron DJ, Kostuk WJ, Knudtson M, Dada M, Casperson P, Harris CL, Chaitman BR, et al. COURAGE Trial Research Group. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med. 2007;356:1503–1516. doi: 10.1056/NEJMoa070829. - DOI - PubMed
-
- Bech GJ, De Bruyne B, Pijls NH, de Muinck ED, Hoorntje JC, Escaned J, Stella PR, Boersma E, Bartunek J, Koolen JJ, Wijns W. Fractional flow reserve to determine the appropriateness of angioplasty in moderate coronary stenosis: a randomized trial. Circulation. 2001;103:2928–2934. - PubMed
-
- Tonino PA, De Bruyne B, Pijls NH, Siebert U, Ikeno F, van’ t Veer M, Klauss V, Manoharan G, Engstrøm T, Oldroyd KG, Ver Lee PN, et al. FAME Study Investigators. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009;360:213–224. doi: 10.1056/NEJMoa0807611. - DOI - PubMed
-
- De Bruyne B, Pijls NH, Kalesan B, Barbato E, Tonino PA, Piroth Z, Jagic N, Möbius-Winkler S, Mobius-Winckler S, Rioufol G, Witt N, et al. FAME 2 Trial Investigators. Fractional flow reserve-guided PCI versus medical therapy in stable coronary disease. N Engl J Med. 2012;367:991–1001. doi: 10.1056/NEJMoa1205361. - DOI - PubMed
-
- Tonino PA, Fearon WF, De Bruyne B, Oldroyd KG, Leesar MA, Ver Lee PN, Maccarthy PA, Van’t Veer M, Pijls NH. Angiographic versus functional severity of coronary artery stenoses in the FAME study fractional flow reserve versus angiography in multivessel evaluation. J Am Coll Cardiol. 2010;55:2816–2821. doi: 10.1016/j.jacc.2009.11.096. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
