

Natural history of multiple system atrophy in the USA: a prospective cohort study
- PMID: 26025783
- PMCID: PMC4472464
- DOI: 10.1016/S1474-4422(15)00058-7
Natural history of multiple system atrophy in the USA: a prospective cohort study
Abstract
Background: Multiple system atrophy is a rare, fatal neurodegenerative disorder with symptoms of autonomic failure plus parkinsonism, cerebellar ataxia, or both. We report results of the first prospective natural history study of multiple system atrophy in the USA, and the effects of phenotype and autonomic failure on prognosis.
Methods: We recruited participants with probable multiple system atrophy-of either the parkinsonism subtype (MSA-P) or the cerebellar ataxia subtype (MSA-C)-at 12 neurology centres in the USA specialising in movement or autonomic disorders. We followed up patients every 6 months for 5 years and assessed them with the Unified Multiple System Atrophy Rating Scale part I (UMSARS I; a functional score of symptoms and ability to undertake activities of daily living), UMSARS II (neurological motor evaluation), and the Composite Autonomic Symptoms Scale (COMPASS)-select (a measure of autonomic symptoms and autonomic functional status). We assessed potential predictors of outcome. We used Cox proportional hazards models to calculate univariate hazard ratios for shorter survival using age at disease onset as a continuous variable and sex, clinical phenotype, and early development of neurological and autonomic manifestations as categorical variables.
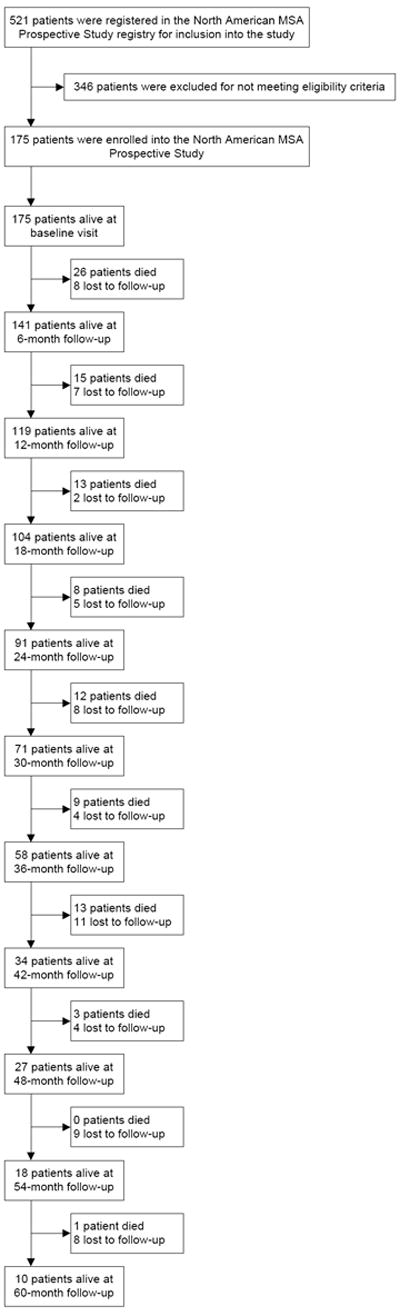
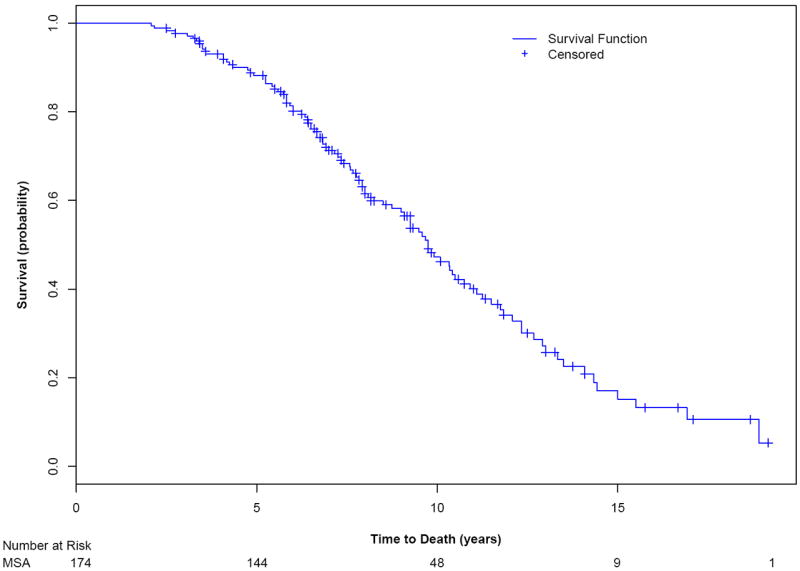
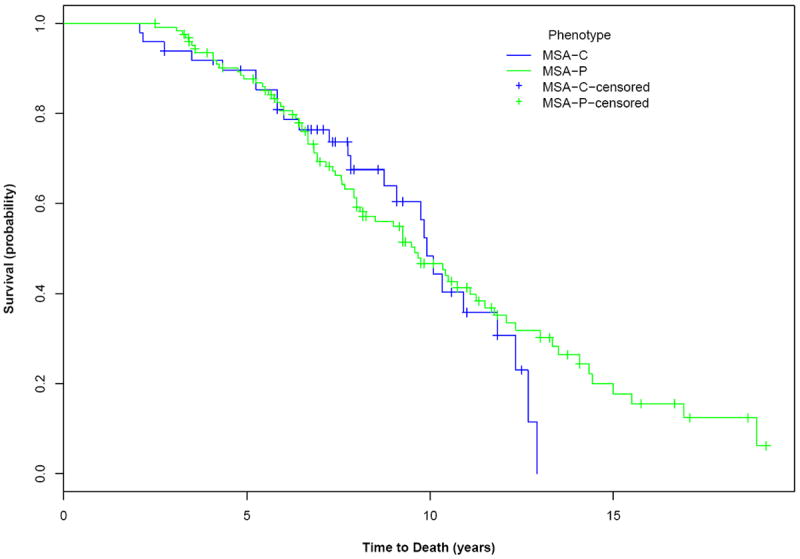
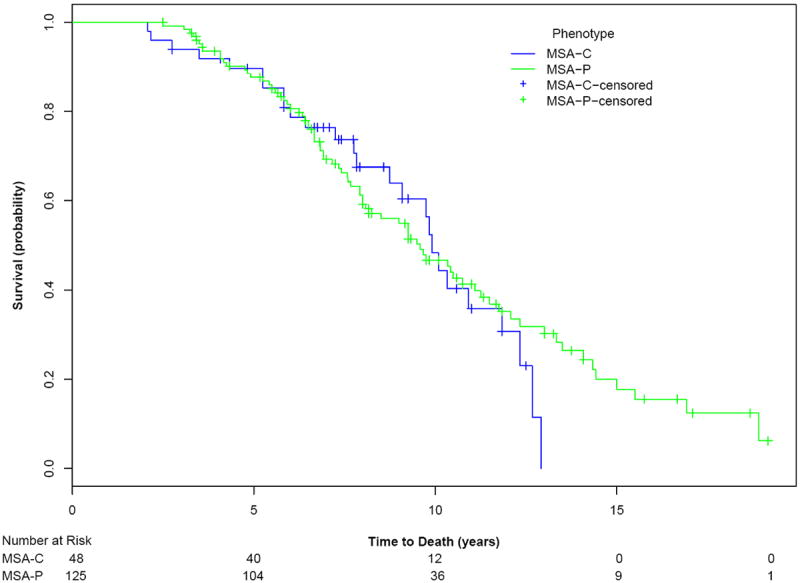
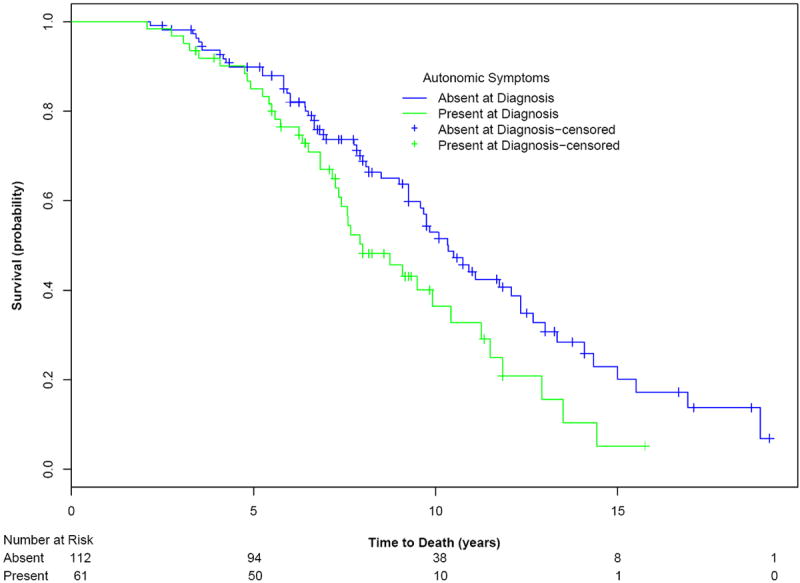
Findings: We recruited 175 participants. Mean age at study entry was 63·4 years (SD 8·6). Median survival from symptom onset was 9·8 years (95% CI 8·8-10·7) and median survival from enrolment was 1·8 years (0·9-2·7). Participants with severe symptomatic autonomic failure (symptomatic orthostatic hypotension, urinary incontinence, or both) at diagnosis (n=62) had a worse prognosis than those without severe disease (n=113; median survival 8·0 years, 95% CI 6·5-9·5 vs 10·3 years, 9·3-11·4; p=0·021). At baseline, patients with MSA-P (n=126) and MSA-C (n=49) had much the same symptoms and functional status: mean UMSARS I 25·2 (SD 8·08) versus 24·6 (8·34; p=0·835); mean UMSARS II 26·4 (8·8) versus 25·4 (10·5; p=0·764); COMPASS-select 43·5 (18·7) versus 42·8 (19·6; p=0·835). Progression over 5 years, assessed by change in UMSARS I, UMSARS II, and COMPASS-select, was modest.
Interpretation: Probable multiple system atrophy is a late-stage disease with short survival. The natural histories of MSA-P and MSA-C are similar and severe symptomatic autonomic failure at diagnosis is associated with worse prognosis.
Funding: US National Institutes of Health, Mayo Clinic, and Kathy Shih Memorial Foundation.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Phillip A. Low, MD has no conflicts of interest to disclose.
Stephen G. Reich, MD has no conflicts of interest to disclose.
Joseph Jankovic, MD reports grants from Allergan, Inc; Ceregene, Inc; CHDI Foundation; GE
Healthcare; Huntington’s Disease Society of America; Huntington Study Group; Ipsen Limited; Lundbeck Inc; Michael J Fox Foundation for Parkinson Research; Medtronic; Merz Pharmaceuticals; National Institutes of Health; National Parkinson Foundation; St. Jude Medical; Teva Pharmaceutical Industries Ltd; UCB Inc; University of Rochester; Parkinson Study Group, during the conduct of the study; personal fees from Allergan, Inc; Auspex Pharmaceuticals, Inc; Ipsen Biopharmaceuticals, Inc.; Lundbeck Inc; Merz Pharmaceuticals; Teva Pharmaceutical Industries Ltd; UCB Inc; US World Meds., grants from Allergan, Inc; Ceregene, Inc; CHDI Foundation; GE Healthcare; Huntington’s Disease Society of America; Huntington Study Group; Ipsen Limited; Lundbeck Inc; Michael J Fox Foundation for Parkinson Research; Medtronic; Merz Pharmaceuticals; National Institutes of Health; National Parkinson Foundation; St. Jude Medical; Teva Pharmaceutical Industries Ltd; UCB Inc; University of Rochester; Parkinson Study Group, other from Cambridge; Elsevier; Future Science Group; Hodder Arnold; Lippincott Williams and Wilkins; Wiley-Blackwell, outside the submitted work;.
Matthew B. Stern, MD reports Consultant: Teva, Merz, Adamas, Civitas Equity: Civitas, Adamas Officer: International Parkinson and Movement Disorder Society.
Peter Novak, MD has no conflicts of interest to disclose.
Caroline M. Tanner, MD, PhD reports personal fees from Adamas Pharmaceuticals, personal fees from Pfizer Pharmaceuticals, outside the submitted work.
Sid Gilman, MD, FRCP has no conflicts of interest to disclose.
Frederick Wooten, MD has no conflicts of interest to disclose.
Brad Racette, MD has no conflicts of interest to disclose.
Thomas Chelimsky, MD reports grants from NIH-NIDDK, other from Ironwood Pharmaceuticals, outside the submitted work.
Wolfgang Singer, MD has no conflicts of interest to disclose.
David M. Sletten, MBA has no conflicts of interest to disclose.
Paola Sandroni, MD has no conflicts of interest to disclose.
Jay Mandrekar, PhD has no conflicts of interest to disclose.
Figures
Comment in
-
Multiple system atrophy in the USA: another piece in the jigsaw.Lancet Neurol. 2015 Jul;14(7):672-4. doi: 10.1016/S1474-4422(15)00090-3. Epub 2015 May 27. Lancet Neurol. 2015. PMID: 26025782 No abstract available.
-
Neurodegenerative disease: Multiple system atrophy-new insight from prospective studies.Nat Rev Neurol. 2015 Aug;11(8):430-1. doi: 10.1038/nrneurol.2015.124. Epub 2015 Jul 21. Nat Rev Neurol. 2015. PMID: 26195260 No abstract available.
References
-
- Wenning GK, Colosimo C, Geser F, Poewe W. Multiple system atrophy. Lancet Neurol. 2004;3:93–103. - PubMed
-
- Bower JH, Maraganore DM, McDonnell SK, Rocca WA. Incidence of progressive supranuclear palsy and multiple system atrophy in Olmsted County, Minnesota, 1976 to 1990. Neurology. 1997;49:1284–8. - PubMed
-
- Gilman S, Low PA, Quinn N, Albanese A, Ben-Schlomo Y, Fowler CJ, et al. Consensus statement on the diagnosis of multiple system atrophy. J Auton Nerv Syst. 1998;74:189–92. - PubMed
