

A Randomized, Controlled Trial of Cavity Shave Margins in Breast Cancer
- PMID: 26028131
- PMCID: PMC5584380
- DOI: 10.1056/NEJMoa1504473
A Randomized, Controlled Trial of Cavity Shave Margins in Breast Cancer
Abstract
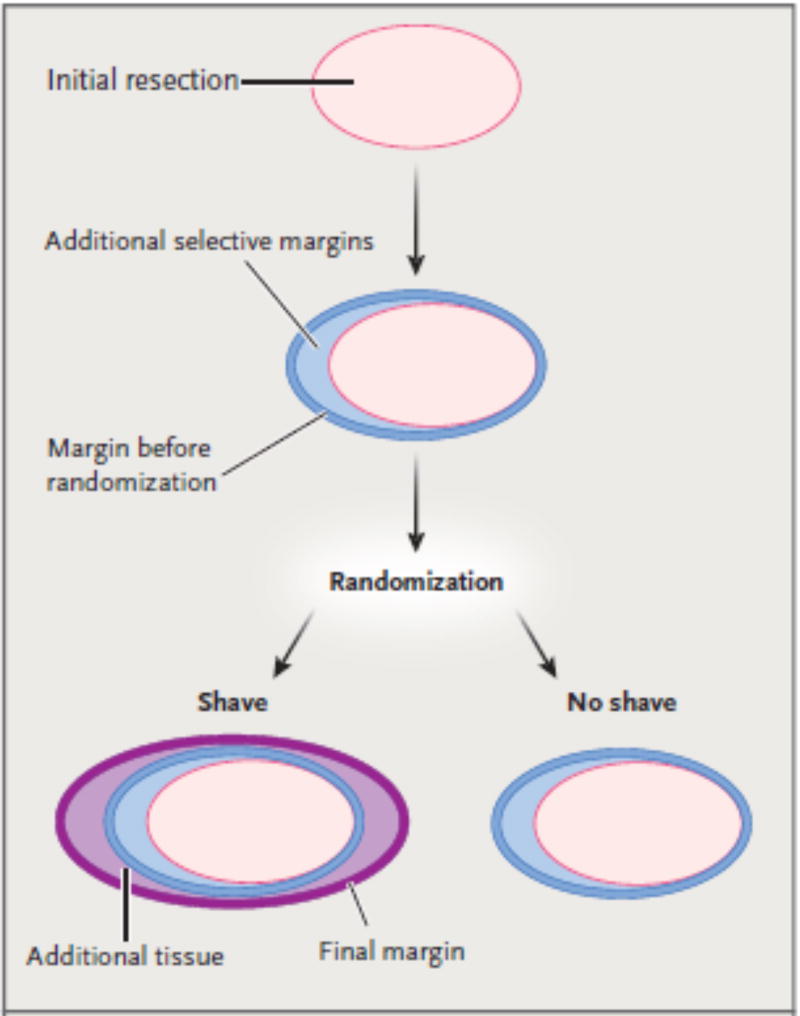
Background: Routine resection of cavity shave margins (additional tissue circumferentially around the cavity left by partial mastectomy) may reduce the rates of positive margins (margins positive for tumor) and reexcision among patients undergoing partial mastectomy for breast cancer.
Methods: In this randomized, controlled trial, we assigned, in a 1:1 ratio, 235 patients with breast cancer of stage 0 to III who were undergoing partial mastectomy, with or without resection of selective margins, to have further cavity shave margins resected (shave group) or not to have further cavity shave margins resected (no-shave group). Randomization occurred intraoperatively after surgeons had completed standard partial mastectomy. Positive margins were defined as tumor touching the edge of the specimen that was removed in the case of invasive cancer and tumor that was within 1 mm of the edge of the specimen removed in the case of ductal carcinoma in situ. The rate of positive margins was the primary outcome measure; secondary outcome measures included cosmesis and the volume of tissue resected.
Results: The median age of the patients was 61 years (range, 33 to 94). On final pathological testing, 54 patients (23%) had invasive cancer, 45 (19%) had ductal carcinoma in situ, and 125 (53%) had both; 11 patients had no further disease. The median size of the tumor in the greatest diameter was 1.1 cm (range, 0 to 6.5) in patients with invasive carcinoma and 1.0 cm (range, 0 to 9.3) in patients with ductal carcinoma in situ. Groups were well matched at baseline with respect to demographic and clinicopathological characteristics. The rate of positive margins after partial mastectomy (before randomization) was similar in the shave group and the no-shave group (36% and 34%, respectively; P=0.69). After randomization, patients in the shave group had a significantly lower rate of positive margins than did those in the no-shave group (19% vs. 34%, P=0.01), as well as a lower rate of second surgery for margin clearance (10% vs. 21%, P=0.02). There was no significant difference in complications between the two groups.
Conclusions: Cavity shaving halved the rates of positive margins and reexcision among patients with partial mastectomy. (Funded by the Yale Cancer Center; ClinicalTrials.gov number, NCT01452399.).
Figures
Comment in
-
Reexcision--The Other Breast Cancer Epidemic.N Engl J Med. 2015 Aug 6;373(6):568-9. doi: 10.1056/NEJMe1507190. N Engl J Med. 2015. PMID: 26244311 No abstract available.
-
Cavity Shave Margins in Breast Cancer.N Engl J Med. 2015 Nov 26;373(22):2187-8. doi: 10.1056/NEJMc1511344. N Engl J Med. 2015. PMID: 26605934 No abstract available.
-
Cavity Shave Margins in Breast Cancer.N Engl J Med. 2015 Nov 26;373(22):2186. doi: 10.1056/NEJMc1511344. N Engl J Med. 2015. PMID: 26605935 No abstract available.
-
Cavity Shave Margins in Breast Cancer.N Engl J Med. 2015 Nov 26;373(22):2186-7. doi: 10.1056/NEJMc1511344. N Engl J Med. 2015. PMID: 26605936 No abstract available.
-
Cavity Shave Margins in Breast Cancer.N Engl J Med. 2015 Nov 26;373(22):2187. doi: 10.1056/NEJMc1511344. N Engl J Med. 2015. PMID: 26605937 No abstract available.
References
-
- Kummerow KL, Du L, Penson DF, Shyr Y, Hooks MA. Nationwide trends in mastectomy for early-stage breast cancer. JAMA Surg. 2015;150:9–16. - PubMed
-
- Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 2002;347:1233–41. - PubMed
-
- Wilke LG, Czechura T, Wang C, et al. Repeat surgery after breast conservation for the treatment of stage 0 to II breast carcinoma: a report from the National Cancer Data Base, 2004–2010. JAMA Surg. 2014;149:1296–305. - PubMed
-
- McCahill LE, Single RM, Aiello Bowles EJ, et al. Variability in reexcision following breast conservation surgery. JAMA. 2012;307:467–75. - PubMed
-
- Moran MS, Schnitt SJ, Giuliano AE, et al. Society of Surgical Oncology-American Society for Radiation Oncology consensus guideline on margins for breast-conserving surgery with whole-breast irradiation in stages I and II invasive breast cancer. Ann Surg Oncol. 2014;21:704–16. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical