

Estimated glomerular filtration rate and albuminuria for prediction of cardiovascular outcomes: a collaborative meta-analysis of individual participant data
- PMID: 26028594
- PMCID: PMC4594193
- DOI: 10.1016/S2213-8587(15)00040-6
Estimated glomerular filtration rate and albuminuria for prediction of cardiovascular outcomes: a collaborative meta-analysis of individual participant data
Abstract
Background: The usefulness of estimated glomerular filtration rate (eGFR) and albuminuria for prediction of cardiovascular outcomes is controversial. We aimed to assess the addition of creatinine-based eGFR and albuminuria to traditional risk factors for prediction of cardiovascular risk with a meta-analytic approach.
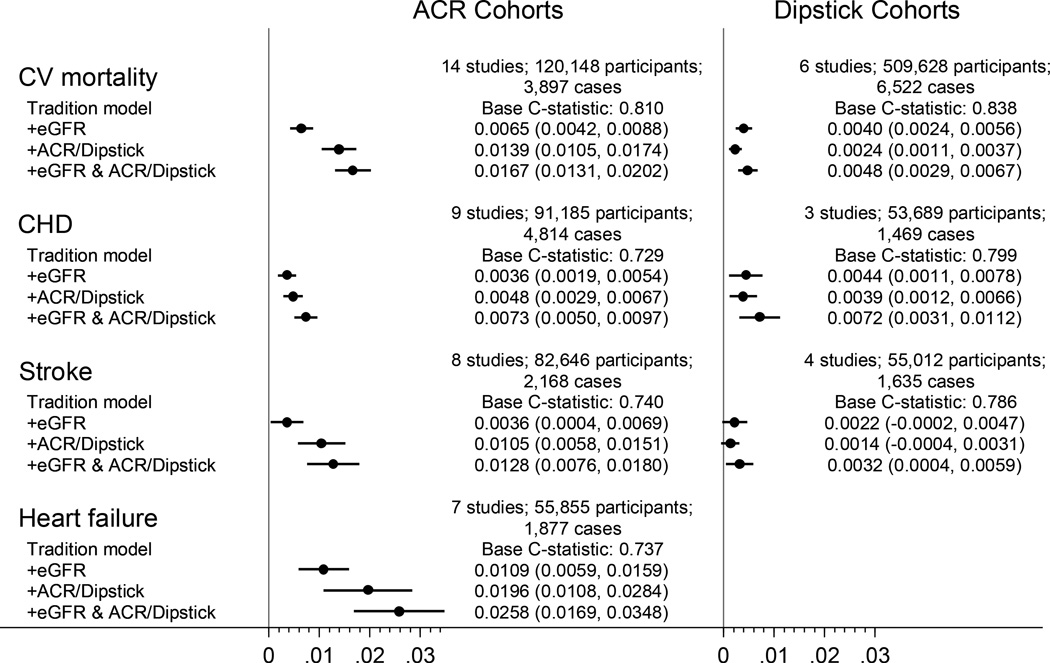
Methods: We meta-analysed individual-level data for 637 315 individuals without a history of cardiovascular disease from 24 cohorts (median follow-up 4·2-19·0 years) included in the Chronic Kidney Disease Prognosis Consortium. We assessed C statistic difference and reclassification improvement for cardiovascular mortality and fatal and non-fatal cases of coronary heart disease, stroke, and heart failure in a 5 year timeframe, contrasting prediction models for traditional risk factors with and without creatinine-based eGFR, albuminuria (either albumin-to-creatinine ratio [ACR] or semi-quantitative dipstick proteinuria), or both.
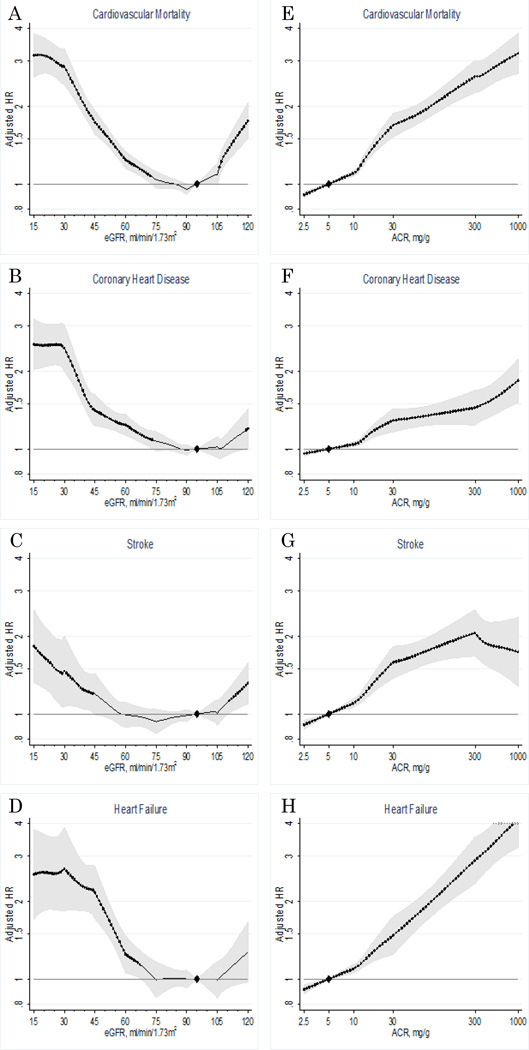
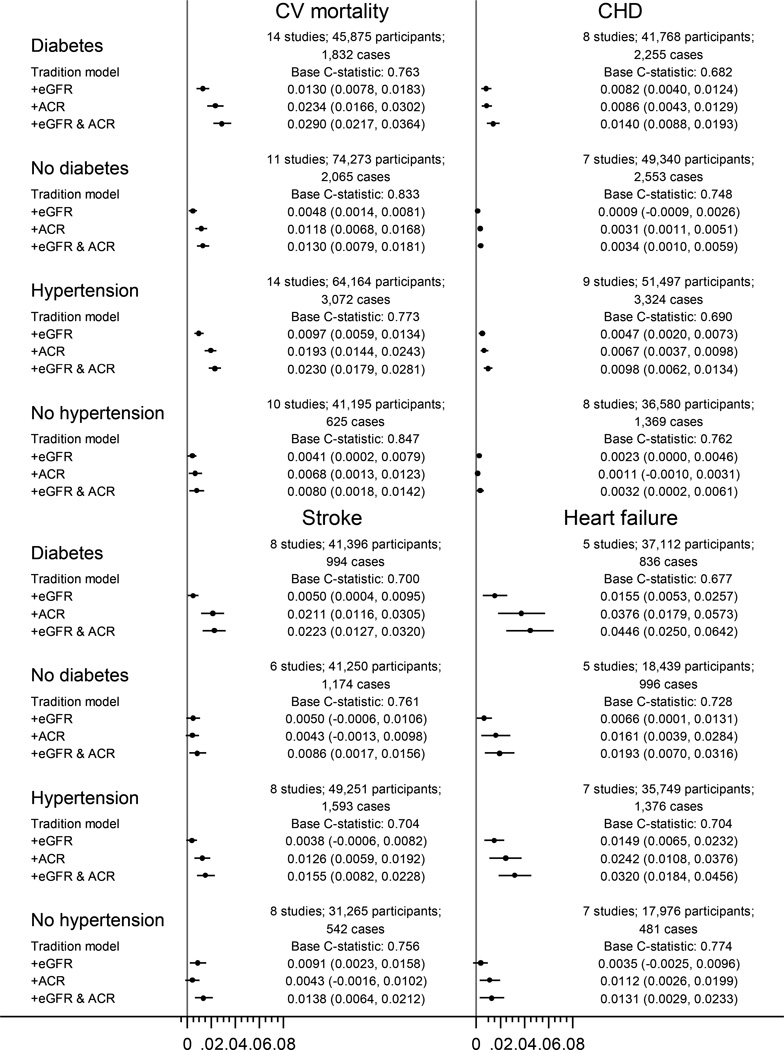
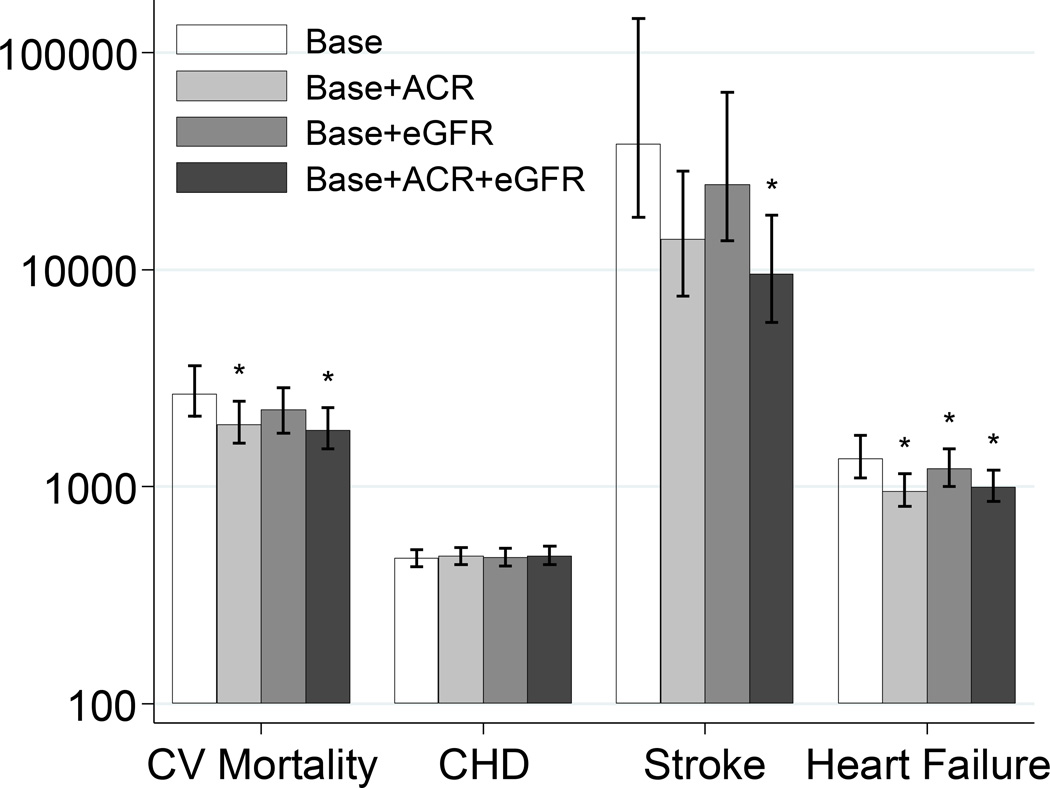
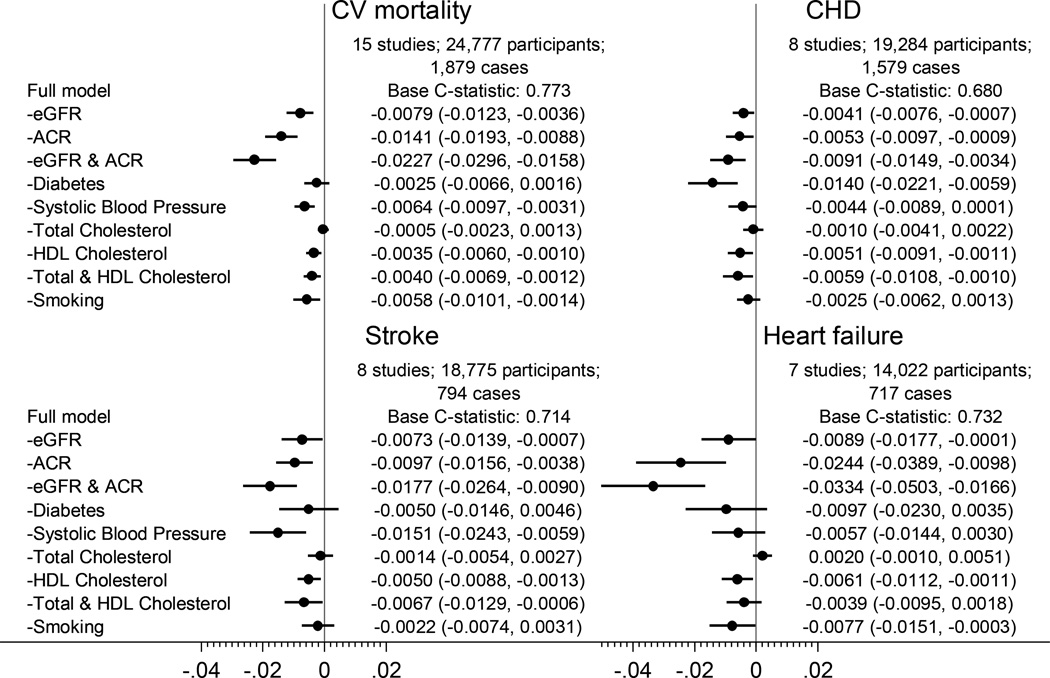
Findings: The addition of eGFR and ACR significantly improved the discrimination of cardiovascular outcomes beyond traditional risk factors in general populations, but the improvement was greater with ACR than with eGFR, and more evident for cardiovascular mortality (C statistic difference 0·0139 [95% CI 0·0105-0·0174] for ACR and 0·0065 [0·0042-0·0088] for eGFR) and heart failure (0·0196 [0·0108-0·0284] and 0·0109 [0·0059-0·0159]) than for coronary disease (0·0048 [0·0029-0·0067] and 0·0036 [0·0019-0·0054]) and stroke (0·0105 [0·0058-0·0151] and 0·0036 [0·0004-0·0069]). Dipstick proteinuria showed smaller improvement than ACR. The discrimination improvement with eGFR or ACR was especially evident in individuals with diabetes or hypertension, but remained significant with ACR for cardiovascular mortality and heart failure in those without either of these disorders. In individuals with chronic kidney disease, the combination of eGFR and ACR for risk discrimination outperformed most single traditional predictors; the C statistic for cardiovascular mortality fell by 0·0227 (0·0158-0·0296) after omission of eGFR and ACR compared with less than 0·007 for any single modifiable traditional predictor.
Interpretation: Creatinine-based eGFR and albuminuria should be taken into account for cardiovascular prediction, especially when these measures are already assessed for clinical purpose or if cardiovascular mortality and heart failure are outcomes of interest. ACR could have particularly broad implications for cardiovascular prediction. In populations with chronic kidney disease, the simultaneous assessment of eGFR and ACR could facilitate improved classification of cardiovascular risk, supporting current guidelines for chronic kidney disease. Our results lend some support to also incorporating eGFR and ACR into assessments of cardiovascular risk in the general population.
Funding: US National Kidney Foundation, National Institute of Diabetes and Digestive and Kidney Diseases.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Humble kidneys predict mighty heart troubles.Lancet Diabetes Endocrinol. 2015 Jul;3(7):489-91. doi: 10.1016/S2213-8587(15)00092-3. Epub 2015 May 28. Lancet Diabetes Endocrinol. 2015. PMID: 26028595 No abstract available.
-
Risk factors: The kidneys find a voice in cardiovascular risk prediction.Nat Rev Nephrol. 2015 Sep;11(9):510-2. doi: 10.1038/nrneph.2015.109. Epub 2015 Jul 7. Nat Rev Nephrol. 2015. PMID: 26149837 No abstract available.
-
Improving Cardiovascular Disease Risk Prediction With Albuminuria and Glomerular Filtration Rate.Am J Kidney Dis. 2016 Feb;67(2):179-81. doi: 10.1053/j.ajkd.2015.10.009. Epub 2015 Nov 14. Am J Kidney Dis. 2016. PMID: 26584516 No abstract available.
References
-
- Herzog CA, Asinger RW, Berger AK, Charytan DM, Diez J, Hart RG, et al. Cardiovascular disease in chronic kidney disease. A clinical update from Kidney Disease: Improving Global Outcomes (KDIGO) Kidney Int. 2011;80(6):572–586. - PubMed
-
- Stevens PE, O’Donoghue DJ, de Lusignan S, Van Vlymen J, Klebe B, Middleton R, et al. Chronic kidney disease management in the United Kingdom: NEOERICA project results. Kidney Int. 2007;72(1):92–99. - PubMed
-
- Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE, et al. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet. 2010;375(9731):2073–2081. - PMC - PubMed
-
- Hallan SI, Astor BC, Romundstad S, Aasarod K, Kvenild K, Coresh J. Association of kidney function and albuminuria with cardiovascular mortality in older versus younger individuals; the HUNT II study. Arch Intern Med. 2007;167(22):2490–2496. - PubMed
-
- Nerpin E, Ingelsson E, Riserus U, Sundstrom J, Larsson A, Jobs E, et al. The combined contribution of albuminuria and glomerular filtration rate to the prediction of cardiovascular mortality in elderly men. Nephrol Dial Transplant. 2011;26(9):2820–2827. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- K23 DK067303/DK/NIDDK NIH HHS/United States
- U01 DK035073/DK/NIDDK NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- K23 DK002904/DK/NIDDK NIH HHS/United States
- U10 EY006594/EY/NEI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- P30 DK079626/DK/NIDDK NIH HHS/United States
- R01 AG007181/AG/NIA NIH HHS/United States
- R01 DK073217/DK/NIDDK NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- R01 DK031801/DK/NIDDK NIH HHS/United States
- U01 NS041588/NS/NINDS NIH HHS/United States
- N01 HC095169/HC/NHLBI NIH HHS/United States
- R01 HL080477/HL/NHLBI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- R01 DK100446/DK/NIDDK NIH HHS/United States
- R01 AG028507/AG/NIA NIH HHS/United States
- N01 HC095159/HC/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
