

Review
eCollection 2015 Jun.
Basal cell carcinoma: pathogenesis, epidemiology, clinical features, diagnosis, histopathology, and management
Affiliations
- PMID: 26029015
- PMCID: PMC4445438
Item in Clipboard
Review
Basal cell carcinoma: pathogenesis, epidemiology, clinical features, diagnosis, histopathology, and management
Yale J Biol Med.
.
Abstract
Basal cell carcinoma (BCC) is the most common malignancy. Exposure to sunlight is the most important risk factor. Most, if not all, cases of BCC demonstrate overactive Hedgehog signaling. A variety of treatment modalities exist and are selected based on recurrence risk, importance of tissue preservation, patient preference, and extent of disease. The pathogenesis, epidemiology, clinical features, diagnosis, histopathology, and management of BCC will be discussed in this review.
Keywords: BCC; ED&C; Mohs surgery; basal cell carcinoma; electrodesiccation and curettage; surgical excision.
Figures
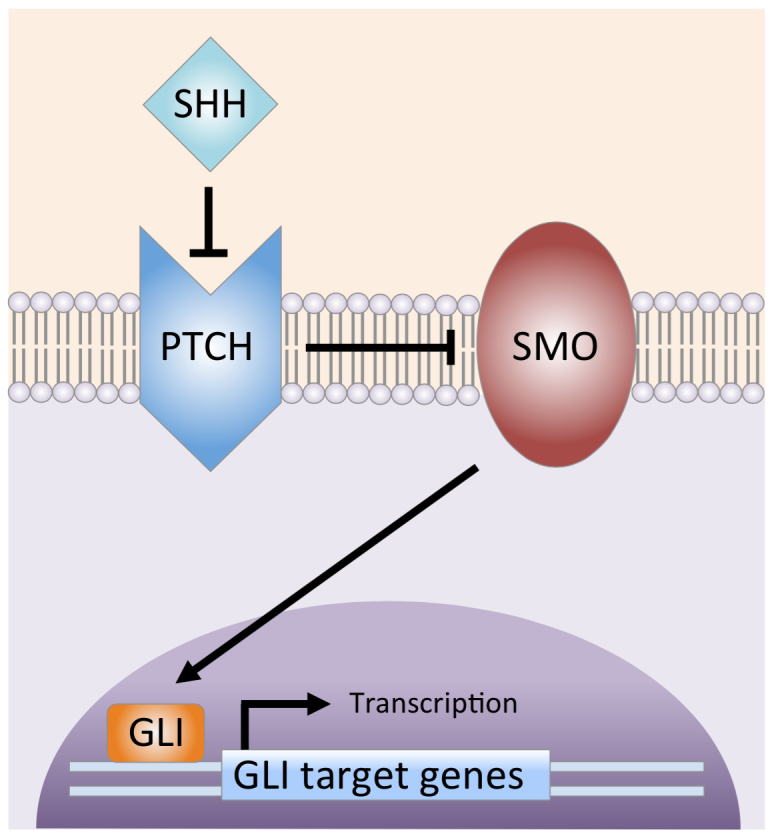
Sonic hedgehog signaling pathway. SHH ligand binds to and inhibits the PTCH transmembrane protein. The inhibition of PTCH relieves suppression of SMO (Smoothened), which then activates the GLI transcription factors. The GLI proteins translocate from the cytoplasm to the nucleus, where they drive gene transcription. (Courtesy of Alexander G. Marzuka, MD)
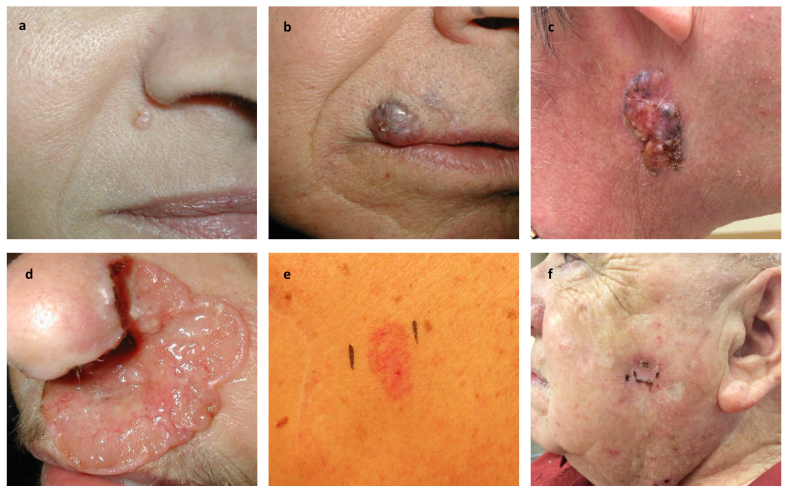
Clinical variants of basal cell carcinoma. a) Nodular basal cell carcinoma with characteristic pearly surface and telangiectasias located lateral to the right alar crease. b) Pigmented variant located on the skin above the right upper lip and extending past the vermilion border into the lip. c) Large nodular basal cell carcinoma with characteristic telangiectasias and pigmented areas on the right side of the neck. d) Ulcerated aggressive basal cell carcinoma, otherwise known as “rodent ulcer.” This basal cell carcinoma spread locally into the nose, causing extensive destruction of the left nasal ala. e) Superficial basal cell carcinoma appearing as a red patch on the trunk. f) Recurrent basal cell carcinoma at the site of ED&C. (Courtesy of Samuel E. Book, MD)
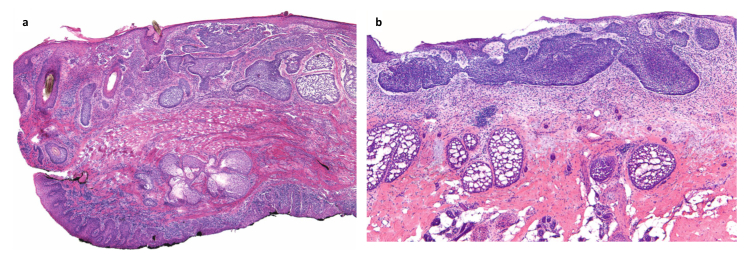
Indolent-growth histologic subtypes [64]. a) Nodular basal cell carcinoma: Medium-power view of a section of eyelid showing both the cutaneous surface at the top and the conjunctiva in the lower inked portion. Nodular basal cell carcinoma is present throughout the dermis. Note the large, nodular aggregates of dark-blue-staining basaloid keratinocytes showing peripheral palisading and clefting. b) Superficial basal cell carcinoma: Medium-power view of superficial basal cell carcinoma, showing basaloid aggregates emanating from the epidermis and growing along an axis parallel to the epidermis. Peripheral palisading and clefting is present.
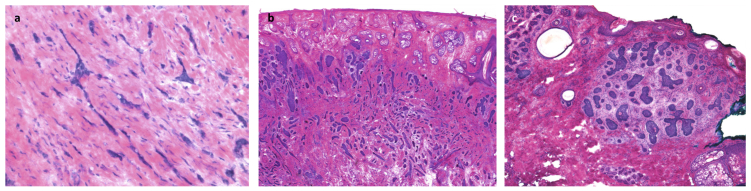
Aggressive-growth histologic subtypes [64]. a) Morpheaform basal cell carcinoma: High-power view of small irregular (sharply angulated) tongues of basaloid, neoplastic cells, ranging from one to four cells thick, embedded within a heavily collagenized stroma. b) Infiltrative basal cell carcinoma: Low-power view of basaloid aggregates of various sizes and shapes, many with angulated appearance, that decrease in size from superficial to the deep portion of the neoplasm. c) Micronodular basal cell carcinoma: small, nodular, irregular aggregates of basaloid neoplastic cells surrounded by cellular myxoid stroma. Focal clefting is appreciated between the neoplastic aggregates and the stroma.
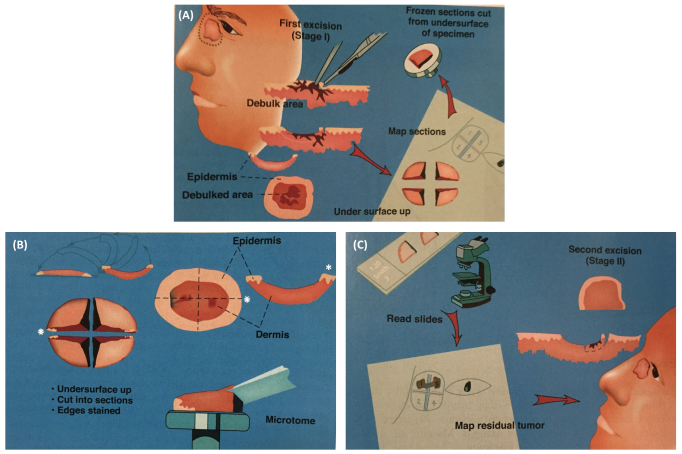
Mohs micrographically controlled surgery (MCCS). A) After gentle curettage for debulking of the tumor, the lesion is excised with a minimal margin of clinically normal-appearing tissue and the specimen is precisely mapped and processed immediately by frozen section for microscopic examination. B) The whole specimen is transected, inverted, and inked. The white asterisks indicate the 3 o’clock position of the lateral margin. Each segment of the whole specimen is processed by frozen section with the use of a microtome, which cuts from the undersurface of the segments. C) The deep and lateral margins of each segment are viewed with a microscope in search for the presence of tumor cells (positive margin). Precise mapping allows for directed extirpation of any remaining tumor. (Courtesy of David J. Leffell, MD, Manual of Skin Surgery, Second Edition, PMPH; 2011.)
References
-
- Gorlin RJ, Goltz RW. Multiple nevoid basal-cell epithelioma, jaw cysts and bifid rib. A syndrome. N Engl J Med. 1960;262:908–912. - PubMed
-
- Gailani MR, Bale SJ, Leffell DJ, DiGiovanna JJ, Peck GL, Poliak S. et al. Developmental defects in Gorlin syndrome related to a putative tumor suppressor gene on chromosome 9. Cell. 1992;69(1):111–117. - PubMed
-
- Farndon PA, Del Mastro RG, Evans DG, Kilpatrick MW. Location of gene for Gorlin syndrome. Lancet. 1992;339(8793):581–582. - PubMed
-
- Reis A, Kuster W, Linss G, Gebel E, Hamm H, Fuhrmann W. et al. Localisation of gene for the naevoid basal-cell carcinoma syndrome. Lancet. 1992;339(8793):617. - PubMed
-
- Gailani MR, Leffell DJ, Ziegler A, Gross EG, Brash DE, Bale AE. Relationship between sunlight exposure and a key genetic alteration in basal cell carcinoma. J Natl Cancer Inst. 1996;88(6):349–354. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical