

Artery of Percheron infarction: review of literature with a case report
- PMID: 26029025
- PMCID: PMC4387990
- DOI: 10.2478/raon-2014-0037
Artery of Percheron infarction: review of literature with a case report
Abstract
Background: Clinical features indicating an ischemic infarction in the territory of posterior cerebral circulation require a comprehensive radiologic examination, which is best achieved by a multi-modality imaging approach (computed tomography [CT], CT-perfusion, computed tomography angiography [CTA], magnetic resonance imaging [MRI] and diffusion weighted imaging [DWI]). The diagnosis of an acute ischemic infarction, where the damage of brain tissue may still be reversible, enables selection of appropriate treatment and contributes to a more favourable outcome. For these reasons it is essential to recognize common neurovascular variants in the territory of the posterior cerebral circulation, one of which is the artery of Percheron.
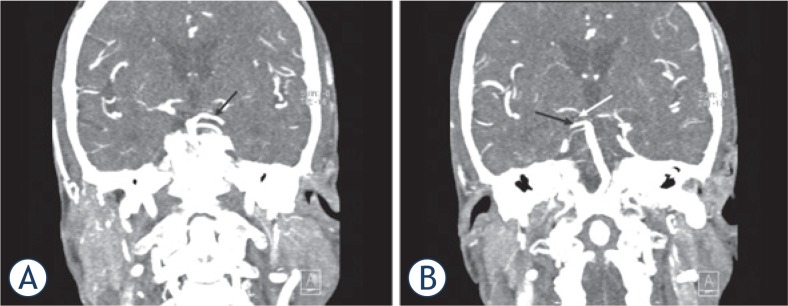
Case report: A 69 year-old woman, last seen awake 10 hours earlier, presented with two typical clinical features of the artery of Percheron infarction, which were vertical gaze palsy and coma. Brain CT and CTA of neck and intracranial arteries upon arrival were interpreted as normal. A new brain CT scan performed 24 hours later revealed hypodensity in the medial parts of thalami. Other imaging modalities were not performed, due to the presumption that the window for the application of effective therapy was over. The diagnosis of an artery of Percheron infarction was therefore made retrospectively with the re-examination of the CTA of neck and intracranial arteries.
Conclusions: A multi-modality imaging approach is necessary in every patient with suspicion of the posterior circulation infarction immediately after the onset of symptoms, especially in cases where primary imaging modalities are unremarkable and clinical features are severe, where follow-up examinations are indicated.
Keywords: Percheron; imaging; infarction.
Figures



References
-
- Krampla W, Schmidbauer B, Hruby W. Iscmaemic stroke of the artery of Percheron. Eur Radiol. 2008;18:192–4. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources