

Audiometric characteristics of hyperacusis patients
- PMID: 26029161
- PMCID: PMC4432660
- DOI: 10.3389/fneur.2015.00105
Audiometric characteristics of hyperacusis patients
Abstract
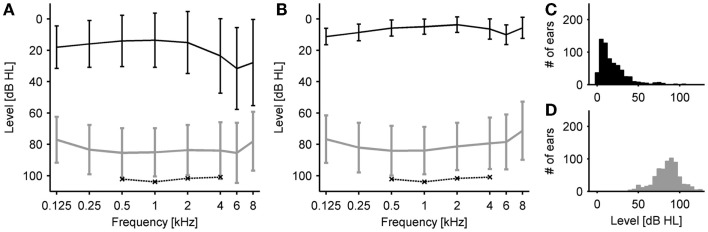
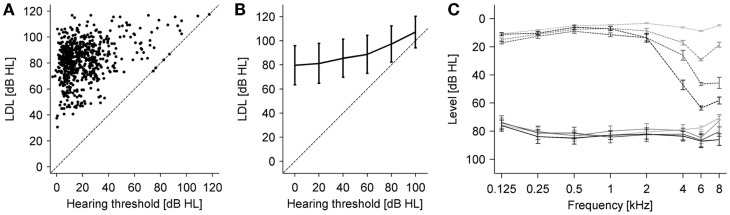
Hyperacusis is a frequent auditory disorder where sounds of normal volume are perceived as too loud or even painfully loud. There is a high degree of co-morbidity between hyperacusis and tinnitus, most hyperacusis patients also have tinnitus, but only about 30-40% of tinnitus patients also show symptoms of hyperacusis. In order to elucidate the mechanisms of hyperacusis, detailed measurements of loudness discomfort levels (LDLs) across the hearing range would be desirable. However, previous studies have only reported LDLs for a restricted frequency range, e.g., from 0.5 to 4 kHz or from 1 to 8 kHz. We have measured audiograms and LDLs in 381 patients with a primary complaint of hyperacusis for the full standard audiometric frequency range from 0.125 to 8 kHz. On average, patients had mild high-frequency hearing loss, but more than a third of the tested ears had normal hearing thresholds (HTs), i.e., ≤20 dB HL. LDLs were found to be significantly decreased compared to a normal-hearing reference group, with average values around 85 dB HL across the frequency range. However, receiver operating characteristic analysis showed that LDL measurements are neither sensitive nor specific enough to serve as a single test for hyperacusis. There was a moderate positive correlation between HTs and LDLs (r = 0.36), i.e., LDLs tended to be higher at frequencies where hearing loss was present, suggesting that hyperacusis is unlikely to be caused by HT increase, in contrast to tinnitus for which hearing loss is a main trigger. Moreover, our finding that LDLs are decreased across the full range of audiometric frequencies, regardless of the pattern or degree of hearing loss, indicates that hyperacusis might be due to a generalized increase in auditory gain. Tinnitus on the other hand is thought to be caused by neuroplastic changes in a restricted frequency range, suggesting that tinnitus and hyperacusis might not share a common mechanism.
Keywords: audiogram; hearing loss; hyperacusis; loudness discomfort levels; tinnitus.
Figures


References
-
- Vernon JA. Pathophysiology of tinnitus: a special case – hyperacusis and a proposed treatment. Am J Otol (1987) 8:201–2. - PubMed
-
- Baguley D, Andersson G. Hyperacusis: Mechanisms, Diagnosis, and Therapies. San Diego, CA: Plural Pub; (2007).
-
- Jastreboff PJ, Hazell JWP. Tinnitus Retraining Therapy: Implementing the Neurophysiological Model. Cambridge: Cambridge University Press; (2004).
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous