

Bricker versus Wallace anastomosis: A meta-analysis of ureteroenteric stricture rates after ileal conduit urinary diversion
- PMID: 26029296
- PMCID: PMC4439225
- DOI: 10.5489/cuaj.2692
Bricker versus Wallace anastomosis: A meta-analysis of ureteroenteric stricture rates after ileal conduit urinary diversion
Abstract
Introduction: Data comparing the incidence of ureteroenteric strictures for Bricker and Wallace anastomoses are limited. This study compares both anastomotic techniques in terms of ureteroenteric stricture rates after radical cystectomy and ileal conduit urinary diversion.
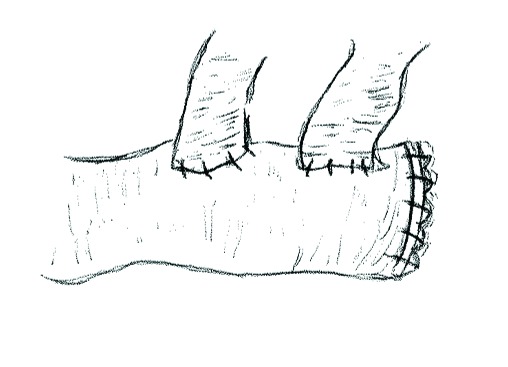
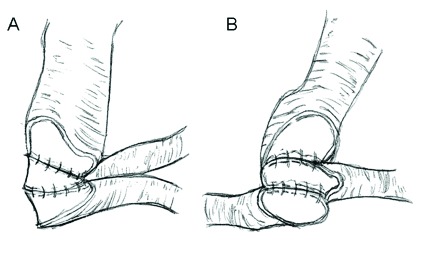
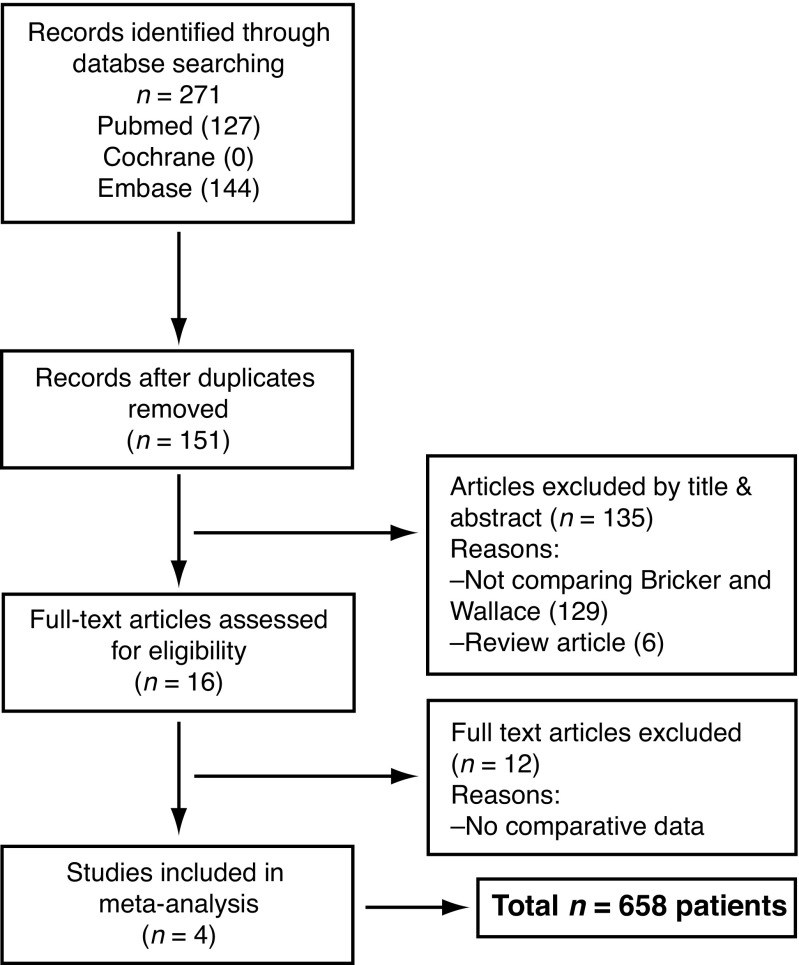
Methods: Electronic databases (Medline, EMBASE, and Cochrane database) were searched for studies comparing Bricker and Wallace ureteroeneteric anastomoses for ileal conduit urinary diversion after radical cystectomy. Meta-analyses were performed using the random effects method. The primary outcome measure was to determine differences in postoperative ureteroenteric stricture rates for both surgical techniques. Four studies describing 658 patients met the inclusion criteria. The total number of ureters used for ureteroeneteric anastomoses was 1217 (545 in the Bricker group and 672 in the Wallace group).
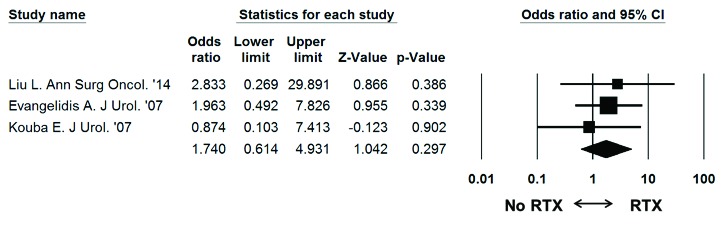
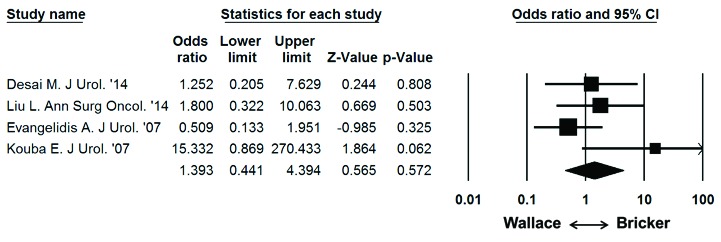
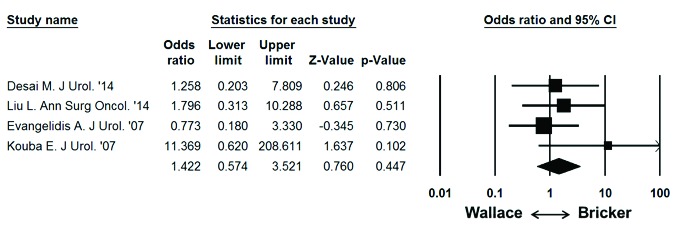
Results: There were no significant differences in age (p = 0.472), gender (p = 0.897), duration of follow-up (p = 0.168), and duration to stricture development between groups (p = 0.439). The overall stricture rate was 29 of 1217 (2.4%); 16 of 545 ureters (2.9%) in the Bricker group and 13 of 672 ureters (1.9%) in the Wallace group. The Bricker anastomosis was not associated with a significantly higher overall stricture rate compared to the Wallace ureteroenteric anastomosis (odds ratio: 1.393, 95% confidence interval: 0.441-4.394, p = 0.572).
Conclusion: Accepting limitations in the available data, we found no significant difference in the incidence of ureteroenteric stricture for Bricker and Wallace anastomoses.
Figures
References
-
- Bricker EM. Bladder substitution after pelvic evisceration. Surg Clin North Am. 1950;30:1511–21. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
