

Antidepressants for the treatment of depression in people with cancer
- PMID: 26029972
- PMCID: PMC6457578
- DOI: 10.1002/14651858.CD011006.pub2
Antidepressants for the treatment of depression in people with cancer
Update in
-
Antidepressants for the treatment of depression in people with cancer.Cochrane Database Syst Rev. 2018 Apr 23;4(4):CD011006. doi: 10.1002/14651858.CD011006.pub3. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2023 Mar 31;3:CD011006. doi: 10.1002/14651858.CD011006.pub4. PMID: 29683474 Free PMC article. Updated.
Abstract
Background: Major depression and other depressive conditions are common in people with cancer. These conditions are not easily detectable in clinical practice, due to the overlap between medical and psychiatric symptoms, as described by diagnostic manuals such as the Diagnostic and Statistical Manual of Mental Disorders (DSM) and International Classification of Diseases (ICD). Moreover, it is particularly challenging to distinguish between pathological and normal reactions to such a severe illness. Depressive symptoms, even in subthreshold manifestations, have been shown to have a negative impact in terms of quality of life, compliance with anti-cancer treatment, suicide risk and likely even the mortality rate for the cancer itself. Randomised controlled trials (RCTs) on the efficacy and tolerability of antidepressants in this population group are few and often report conflicting results.
Objectives: To assess the effects and acceptability of antidepressants for treating depressive symptoms in adults (18 years or older) with cancer (any site and stage).
Search methods: We searched the following electronic bibliographic databases: the Cochrane Central Register of Controlled Trials (CENTRAL 2014, Issue 3), MEDLINE Ovid (1946 to April week 3, 2014), EMBASE Ovid (1980 to 2014 week 17) and PsycINFO Ovid (1987 to April week 4, 2014). We additionally handsearched the trial databases of the most relevant national, international and pharmaceutical company trial registers and drug-approving agencies for published, unpublished and ongoing controlled trials.
Selection criteria: We included RCTs allocating adults (18 years or above) with any primary diagnosis of cancer and depression (including major depressive disorder, adjustment disorder, dysthymic disorder or depressive symptoms in the absence of a formal diagnosis) comparing antidepressants versus placebo, or antidepressants versus other antidepressants.
Data collection and analysis: Two review authors independently checked eligibility and extracted data using a form specifically designed for the aims of this review. The two authors compared the data extracted and then entered data into RevMan 5 with a double-entry procedure. Information extracted included study and participant characteristics, intervention details, outcome measures for each time point of interest, cost analysis and sponsorship by a drug company. We used the standard methodological procedures expected by The Cochrane Collaboration.
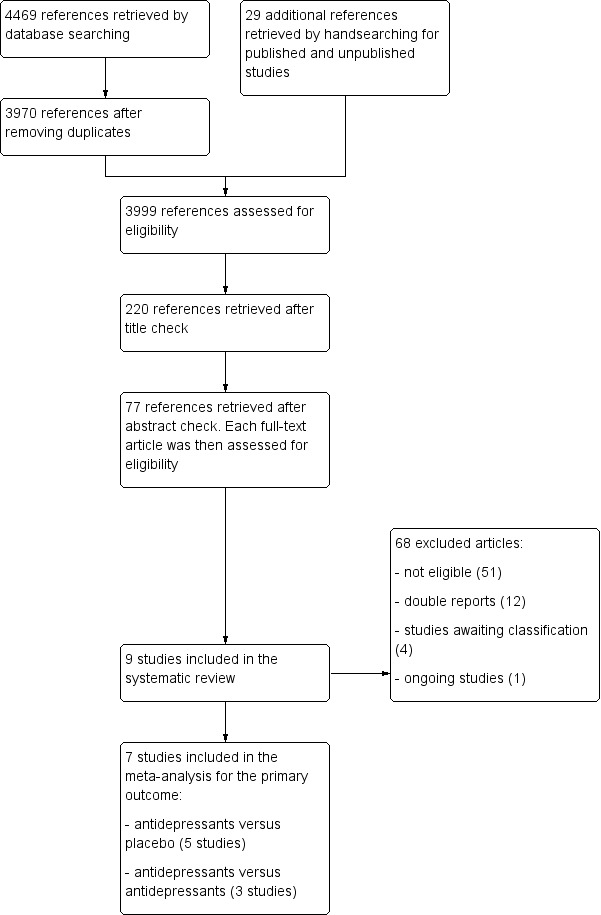
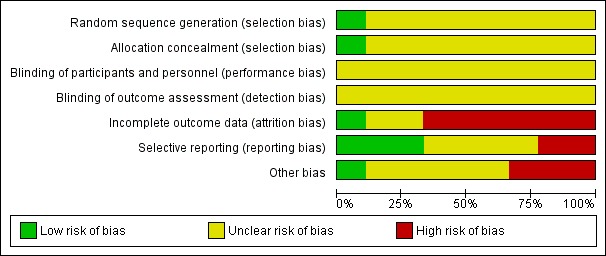
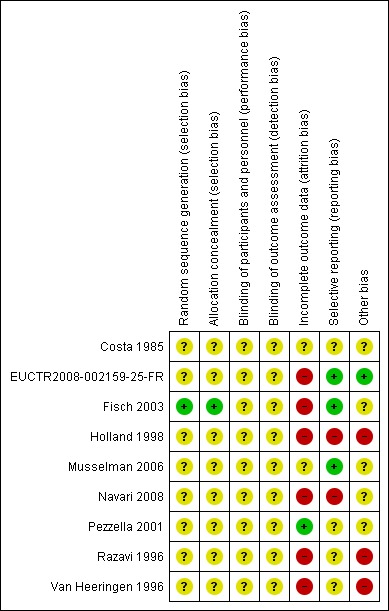
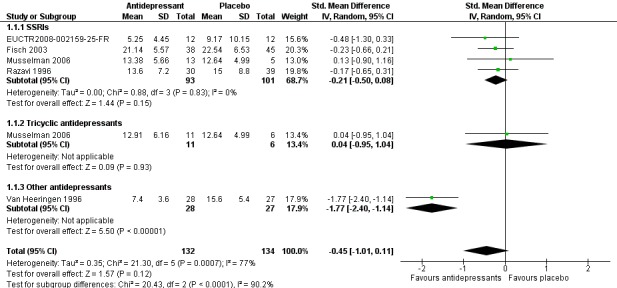
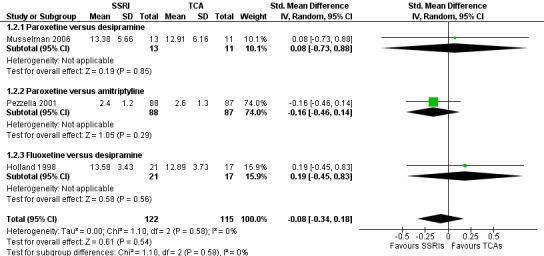
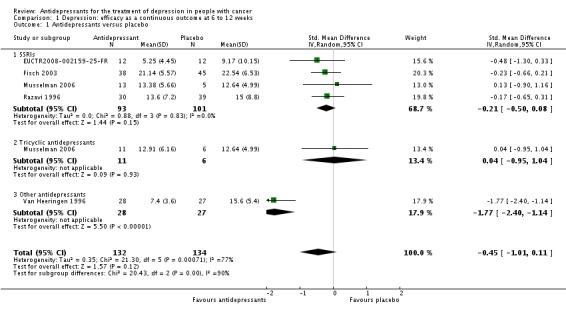
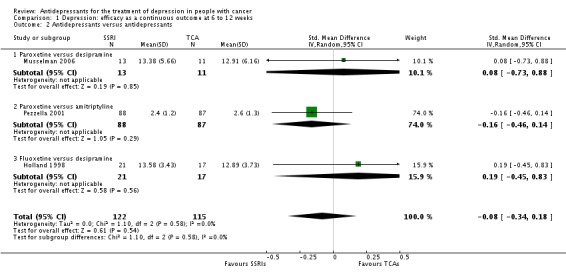
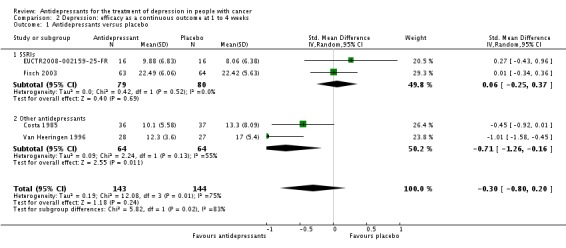
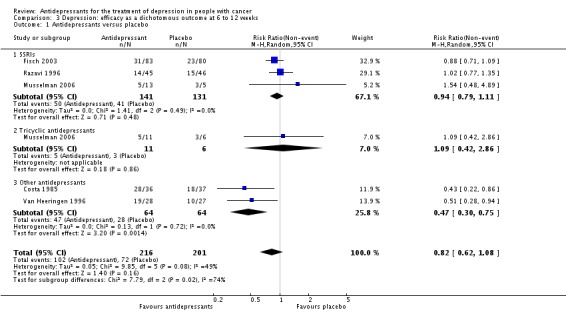
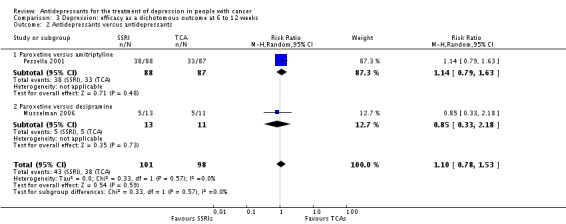
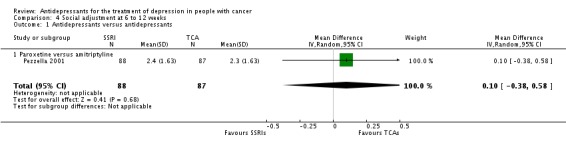
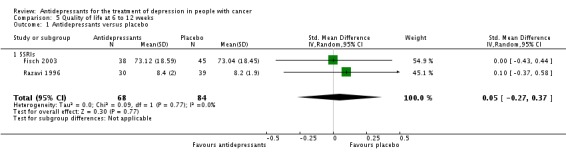
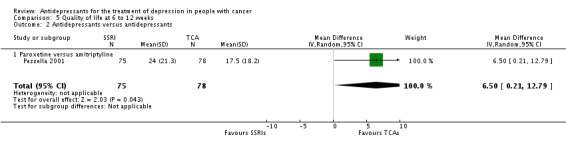
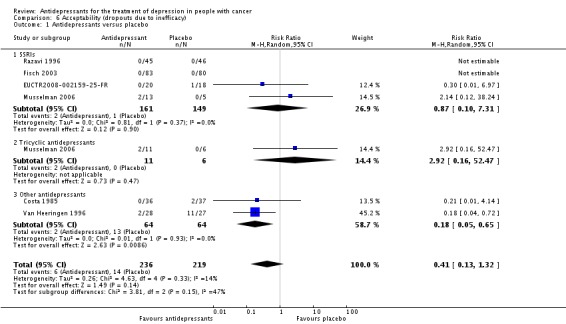
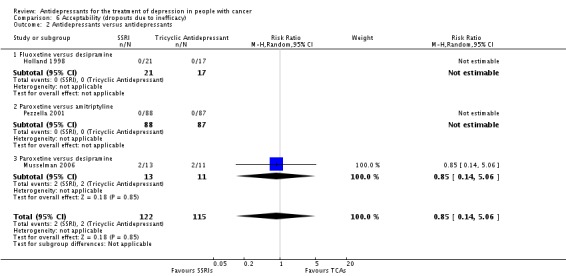
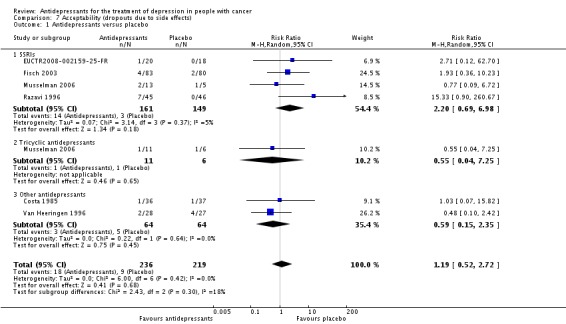
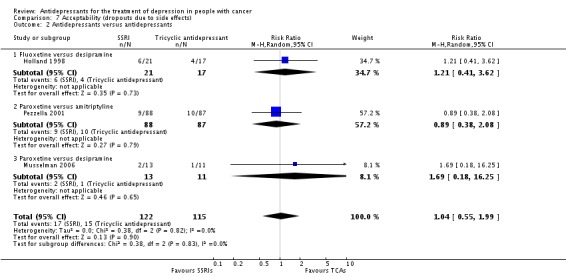
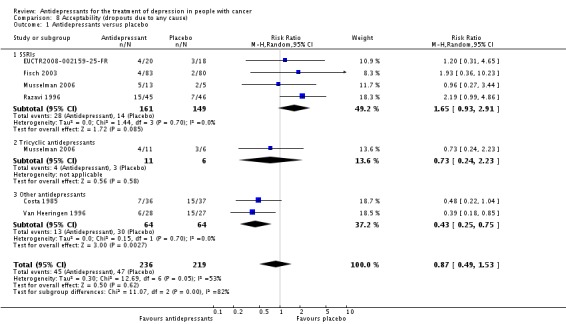
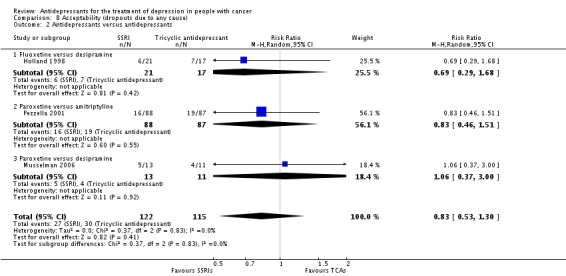
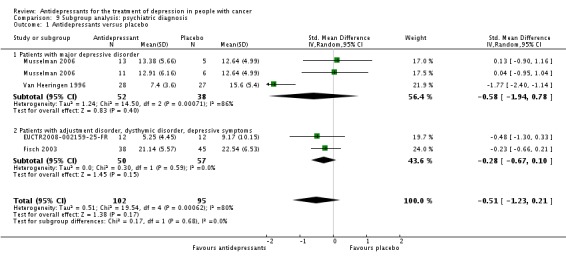
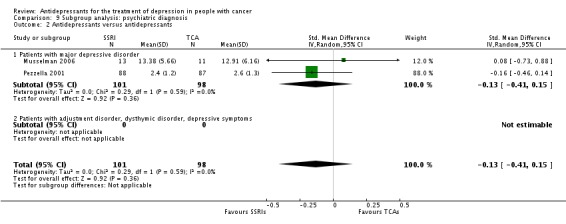
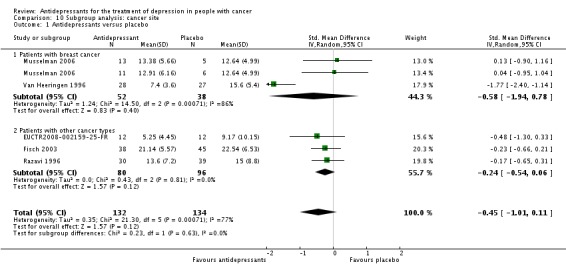
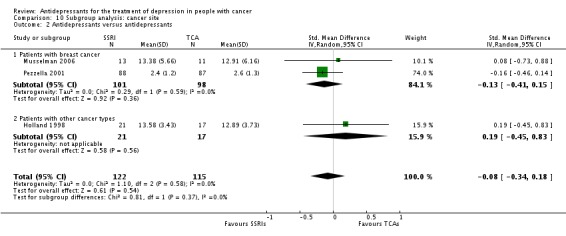
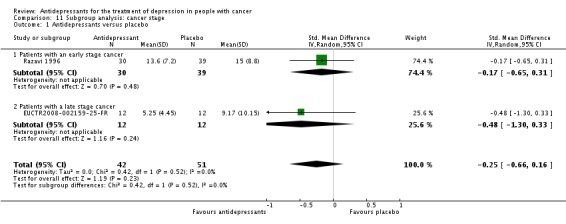
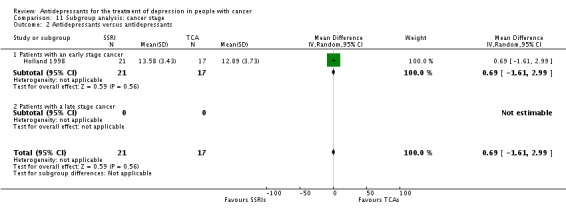
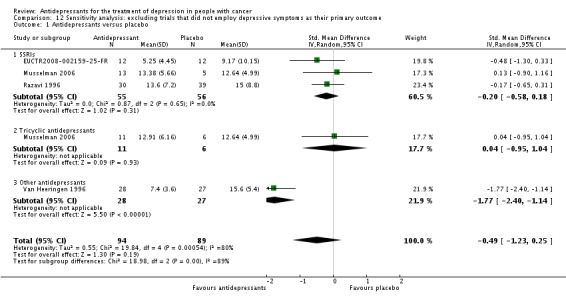
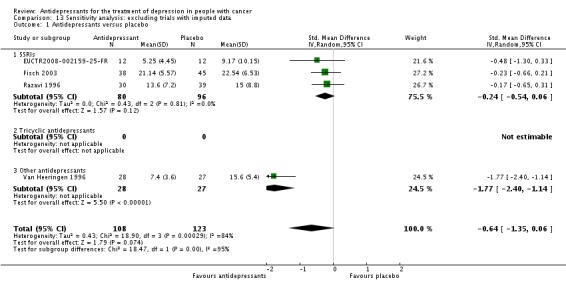
Main results: We retrieved a total of nine studies (861 participants), with seven studies contributing to the meta-analysis for the primary outcome. Four of these compared antidepressants and placebo, two compared two antidepressants and one-three armed study compared two antidepressants and a placebo arm. For the acute phase treatment response (6 to 12 weeks), we found very low quality evidence for the effect of antidepressants as a class on symptoms of depression compared with placebo when measured as a continuous outcome (standardised mean difference (SMD) -0.45, 95% confidence interval (CI) -1.01 to 0.11, five RCTs, 266 participants) or as a proportion of people who had depression (risk ratio (RR) 0.82, 95% CI 0.62 to 1.08, five RCTs, 417 participants). No trials reported data on the follow-up response (more than 12 weeks). In head-to-head comparisons we only retrieved data for selective serotonin reuptake inhibitors (SSRIs) versus tricyclic antidepressants, providing very low quality evidence for the difference between these two classes (SMD -0.08, 95% CI -0.34 to 0.18, three RCTs, 237 participants). No clear evidence of an effect of antidepressants versus either placebo or other antidepressants emerged from the analyses of the secondary efficacy outcomes (dichotomous outcome, response at 6 to 12 weeks, very low quality evidence). We found very low quality evidence for the effect of antidepressants as a class in terms of dropouts due to any cause compared with placebo (RR 0.87, 95% CI 0.49 to 1.53, six RCTs, 455 participants), as well as between SSRIs and tricyclic antidepressants (RR 0.83, 95% CI 0.53 to 1.30, three RCTs, 237 participants). We downgraded the quality of the evidence because the included studies were at an unclear or high risk of bias due to poor reporting, imprecision arising from small sample sizes and wide confidence intervals, and inconsistency due to statistical or clinical heterogeneity.
Authors' conclusions: Despite the impact of depression on people with cancer, available studies were very few and of low quality. This review found very low quality evidence for the effects of these drugs compared with placebo. On the basis of these results clear implications for practice cannot be made. The use of antidepressants in people with cancer should be considered on an individual basis and, considering the lack of head-to-head data, the choice of which agent should be prescribed may be based on the data on antidepressant efficacy in the general population of individuals with major depression, also taking into account that data on medically ill patients suggest a positive safety profile for the SSRIs. Large, simple, randomised, pragmatic trials comparing commonly used antidepressants versus placebo in people with cancer with depressive symptoms, with or without a formal diagnosis of a depressive disorder, are urgently needed to better inform clinical practice.
Conflict of interest statement
Giovanni Ostuzzi ‐ nothing to declare Faith Matcham ‐ nothing to declare Sarah Dauchy ‐ nothing to declare Corrado Barbui ‐ nothing to declare Matthew Hotopf ‐ nothing to declare
SD conducted a multi‐centre trial of participants with cancer and depressive symptoms that compared the efficacy of escitalopram versus placebo. This trial was supported financially by the Institut Gustave‐Roussy and Lundbeck. To prevent bias the author was not involved in assessing the eligibility of the study, or in the extraction of data and quality assessment.
Figures
Comment in
-
[Antidepressants for cancer patients: an individual decision].Dtsch Med Wochenschr. 2015 Sep;140(18):1344. doi: 10.1055/s-0041-103832. Epub 2015 Sep 11. Dtsch Med Wochenschr. 2015. PMID: 26360943 German. No abstract available.
References
References to studies included in this review
-
- Costa D, Mogos I, Toma T. Efficacy and safety of mianserin in the treatment of depression of women with cancer. Acta Psychiatrica Scandinavica 1985;72(Suppl 320):85‐92. - PubMed
-
- Dauchy S, Saltel P, Rey A, Consoli SC, Dolbeault S, Razavi D, et al. A randomized, double‐blind, placebo‐controlled trial of escitalopram for the treatment of emotional distress during treatment for head and neck cancer [Etude randomisée, en double aveugle, contre placebo, de l’Efficacité de l’ Escitalopram dans le traitement de la détresse émotionnelle des sujets atteints de cancer ORL en cours de traitement]. International Clinical Trials Registry Platform2014. [EUCTR2008‐002159‐25‐FR]
-
- Holland JC, Romano SJ, Heiligenstein JH, Tepner RG, Wilson MG. A controlled trial of fluoxetine and desipramine in depressed women with advanced cancer. Psycho‐oncology 1998;7:291–300. - PubMed
-
- Musselman DL, Somerset WI, Guo Y, Manatunga AK, Porter M, Penna S, et al. A double‐blind, multicenter, parallel‐group study of paroxetine, desipramine, or placebo in breast cancer patients (stages I, II, III, and IV) with major depression. Journal of Clinical Psychiatry 2006;67(2):288‐96. - PubMed
References to studies excluded from this review
-
- Biglia N, Torta R, Roagna R, Maggiorotto F, Cacciari F, Ponzone R, et al. Evaluation of low‐dose venlafaxine hydrochloride for the therapy of hot flushes in breast cancer survivors. Maturitas 2005;52(1):78‐85. [PUBMED: 16143229] - PubMed
-
- Biglia N, Sgandurra P, Peano E, Moggio G, Spatola M, Palmisano D. Duloxetine and escitalopram for treatment of hot flushes in breast cancer survivors. Maturitas 2009;63(Suppl 1):S34.
-
- Boekhout AH, Vincent AD, Dalesio OB, Bosch J, Foekema‐Töns JH, Adriaansz S, et al. Management of hot flashes in patients who have breast cancer with venlafaxine and clonidine: a randomized, double‐blind, placebo‐controlled trial. Journal of Clinical Oncology 2011;29(29):3862‐8. [DOI: 10.1200/JCO.2010.33.1298] - DOI - PubMed
-
- Caldera PC, Amodeo L, Borio R, Ramonda E, Torta R. Algorithm‐based treatment for depression in cancer outpatients: efficacy and tolerability evaluation of newer antidepressants. Psycho‐oncology 2009;18(Suppl 2):S317. [DOI: 10.1002/pon.1594] - DOI
References to studies awaiting assessment
-
- Rankin E. Randomised double‐blind placebo controlled trial of venlafaxine in recently diagnosed lung cancer patients: effects on symptom profiles after 12 weeks. controlled‐trials.com2003. [N0405078066]
-
- Miller AA, Shaw EG. Sertraline compared with Hypericum perforatum (St.John's Wort) in treating depression. ClinicalTrials.gov2013. [NCT00066859]
-
- Pirl W. Escitalopram in treating depression in patients with advanced lung or gastrointestinal cancer. ClinicalTrials.gov2012. [NCT00387348]
-
- Nishimura R, Matsushita M. An randomized comparative study of efficacy and safety between mirtazapine and duloxetine hydrochloride in patients with cancer. UMIN Clinical Trials Registry2012. [UMIN000008768]
References to ongoing studies
-
- Yi Ba. Mirtazapine plus gemcitabine versus gemcitabine in metastasis pancreatic cancer. ClincalTrials.gov2012. [NCT01598584]
Additional references
-
- Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The EORTC QLQ‐C30: a quality of life instrument for use in international clinical trials in oncology. Journal of the National Cancer Institute 1993;85(5):365‐75. - PubMed
-
- Anderson IM, Nutt DJ, Deakin JF. Evidence‐based guidelines for treating depressive disorders with antidepressants: a revision of the 1993 British Association for Psychopharmacology guidelines. Journal of Psychopharmacology (Oxford, England) 2000;14(1):3‐20. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous