

Freedom from recurrent ventricular tachycardia after catheter ablation is associated with improved survival in patients with structural heart disease: An International VT Ablation Center Collaborative Group study
- PMID: 26031376
- PMCID: PMC4549209
- DOI: 10.1016/j.hrthm.2015.05.036
Freedom from recurrent ventricular tachycardia after catheter ablation is associated with improved survival in patients with structural heart disease: An International VT Ablation Center Collaborative Group study
Abstract
Background: The impact of catheter ablation of ventricular tachycardia (VT) on all-cause mortality remains unknown.
Objective: The purpose of this study was to examine the association between VT recurrence after ablation and survival in patients with scar-related VT.
Methods: Analysis of 2061 patients with structural heart disease referred for catheter ablation of scar-related VT from 12 international centers was performed. Data on clinical and procedural variables, VT recurrence, and mortality were analyzed. Kaplan-Meier analysis was used to estimate freedom from recurrent VT, transplant, and death. Cox proportional hazards frailty models were used to analyze the effect of risk factors on VT recurrence and mortality.
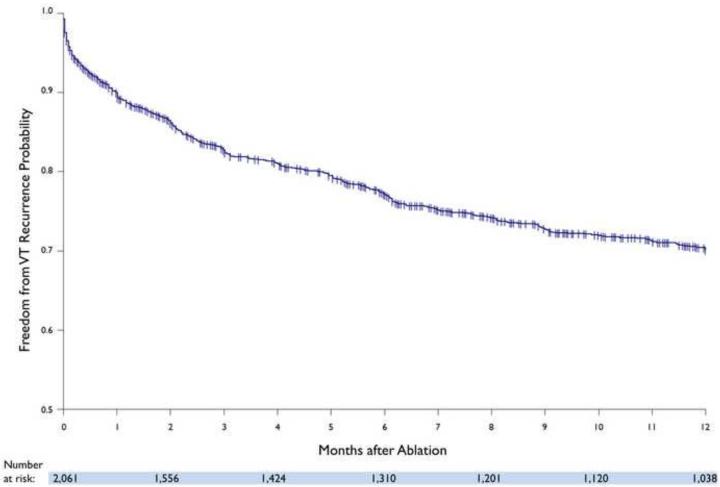
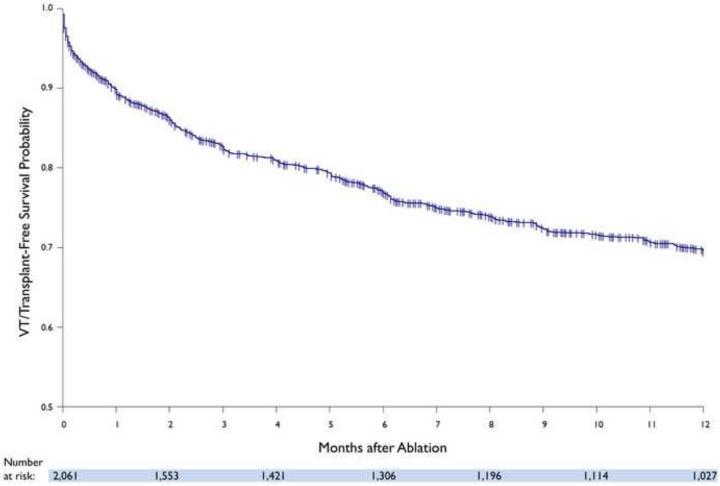
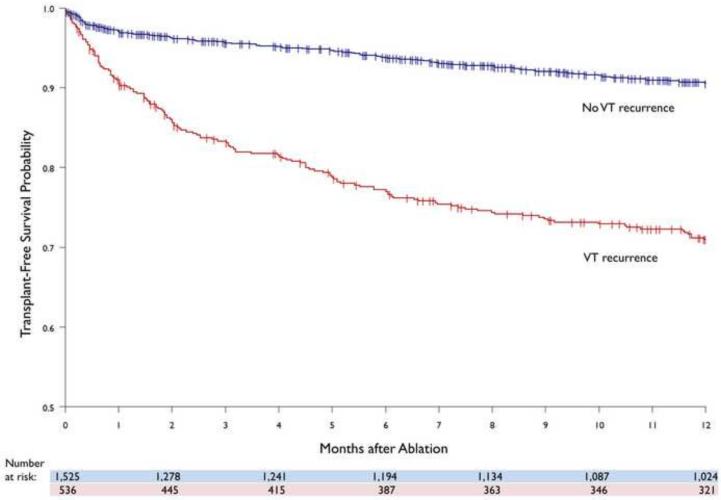
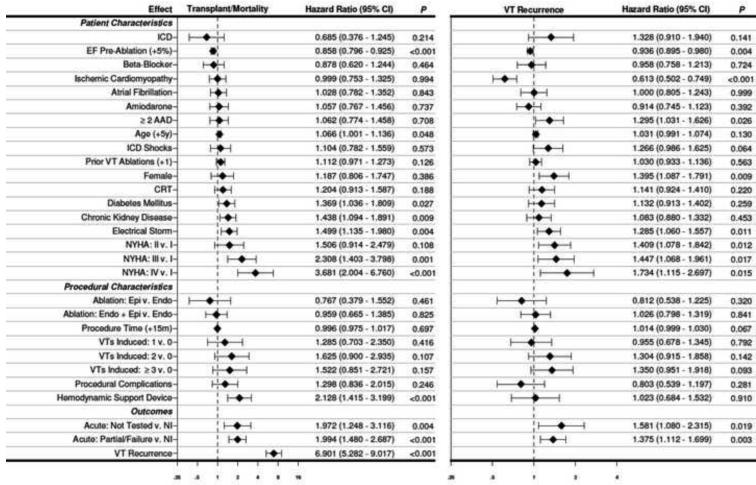
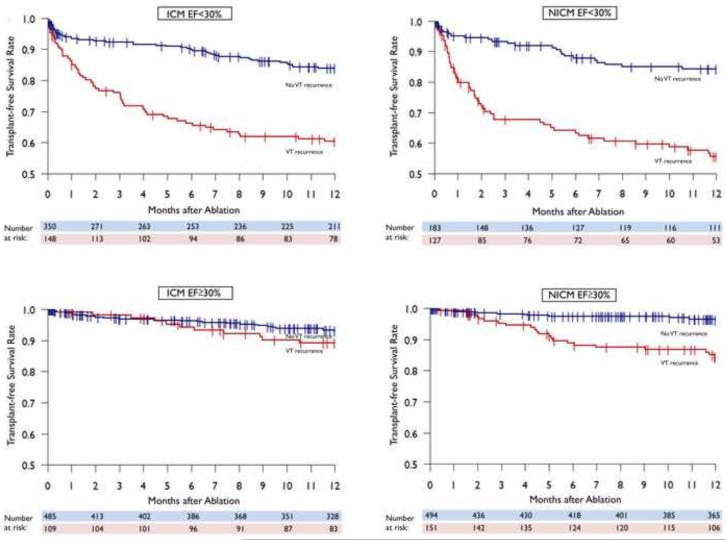
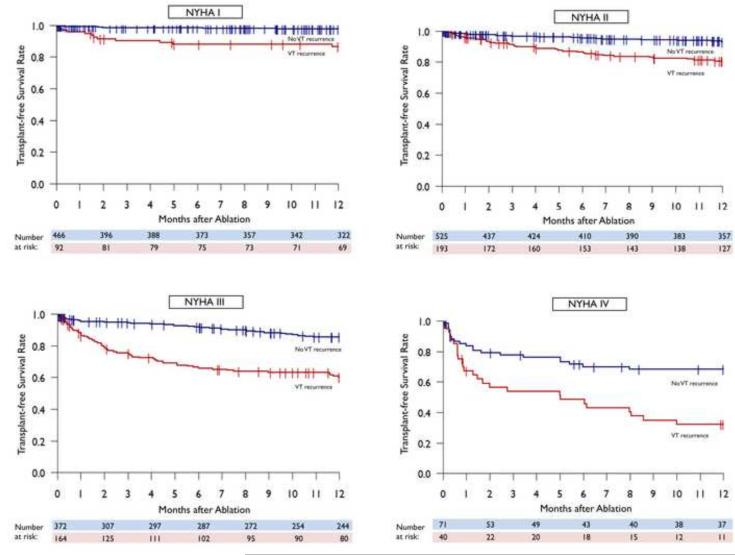
Results: One-year freedom from VT recurrence was 70% (72% in ischemic and 68% in nonischemic cardiomyopathy). Fifty-seven patients (3%) underwent cardiac transplantation, and 216 (10%) died during follow-up. At 1 year, the estimated rate of transplant and/or mortality was 15% (same for ischemic and nonischemic cardiomyopathy). Transplant-free survival was significantly higher in patients without VT recurrence than in those with recurrence (90% vs 71%, P<.001). In multivariable analysis, recurrence of VT after ablation showed the highest risk for transplant and/or mortality [hazard ratio 6.9 (95% CI 5.3-9.0), P<.001]. In patients with ejection fraction <30% and across all New York Heart Association functional classes, improved transplant-free survival was seen in those without VT recurrence.
Conclusion: Catheter ablation of VT in patients with structural heart disease results in 70% freedom from VT recurrence, with an overall transplant and/or mortality rate of 15% at 1 year. Freedom from VT recurrence is associated with improved transplant-free survival, independent of heart failure severity.
Keywords: Ablation; Ventricular tachycardia.
Copyright © 2015 Heart Rhythm Society. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
VT reduction with ablation: A transitive relation to mortality rate?Heart Rhythm. 2015 Sep;12(9):2008-9. doi: 10.1016/j.hrthm.2015.07.009. Epub 2015 Jul 8. Heart Rhythm. 2015. PMID: 26164376 No abstract available.
References
-
- Aliot EM, Stevenson WG, Almendral-Garrote JM, et al. EHRA/HRS Expert Consensus on Catheter Ablation of Ventricular Arrhythmias: developed in a partnership with the European Heart Rhythm Association (EHRA), a Registered Branch of the European Society of Cardiology (ESC), and the Heart Rhythm Society (HRS); in collaboration with the American College of Cardiology (ACC) and the American Heart Association (AHA) Heart Rhythm. 2009;6(6):886–933. - PubMed
-
- Marchlinski FE, Callans DJ, Gottlieb CD, Zado E. Linear ablation lesions for control of unmappable ventricular tachycardia in patients with ischemic and nonischemic cardiomyopathy. Circulation. 2000;101(11):1288–1296. - PubMed
-
- Soejima K, Suzuki M, Maisel WH, Brunckhorst CB, Delacretaz E, Blier L, Tung S, Khan H, Stevenson WG. Catheter ablation in patients with multiple and unstable ventricular tachycardias after myocardial infarction: short ablation lines guided by reentry circuit isthmuses and sinus rhythm mapping. Circulation. 2001;104(6):664–669. - PubMed
-
- Della Bella P, Riva S, Fassini G, Giraldi F, Berti M, Klersy C, Trevisi N. Incidence and significance of pleomorphism in patients with postmyocardial infarction ventricular tachycardia. Acute and long-term outcome of radiofrequency catheter ablation. Eur Heart J. 2004;25(13):1127–1138. - PubMed
-
- Di Biase L, Santangeli P, Burkhardt DJ, et al. Endo-epicardial homogenization of the scar versus limited substrate ablation for the treatment of electrical storms in patients with ischemic cardiomyopathy. J Am Coll Cardiol. 2012;60(2):132–141. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
