

Olfactory identification deficits and increased mortality in the community
- PMID: 26031760
- PMCID: PMC4546561
- DOI: 10.1002/ana.24447
Olfactory identification deficits and increased mortality in the community
Abstract
Objective: To examine the association between odor identification deficits and future mortality in a multiethnic community cohort of older adults.
Methods: Participants were evaluated with the 40-item University of Pennsylvania Smell Identification Test (UPSIT). Follow-up occurred at 2-year intervals with information on death obtained from informant interviews and the National Death Index.
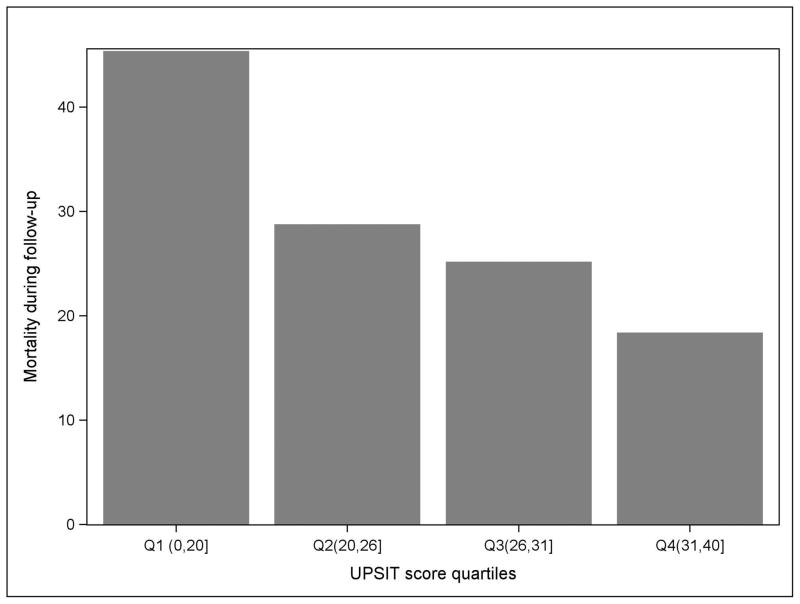
Results: During follow-up (mean = 4.1 years, standard deviation = 2.6), 349 of 1,169 (29.9%) participants died. Participants who died were more likely to be older (p < 0.001), be male (p < 0.001), have lower UPSIT scores (p < 0.001), and have a diagnosis of dementia (p < 0.001). In a Cox model, the association between lower UPSIT score and mortality (hazard ratio [HR] = 1.07 per point interval, 95% confidence interval [CI] = 1.05-1.08, p < 0.001) persisted after controlling for age, gender, education, ethnicity, language, modified Charlson medical comorbidity index, dementia, depression, alcohol abuse, head injury, smoking, body mass index, and vision and hearing impairment (HR = 1.05, 95% CI = 1.03-1.07, p < 0.001). Compared to the fourth quartile with the highest UPSIT scores, HRs for mortality for the first, second, and third quartiles of UPSIT scores were 3.81 (95% CI = 2.71-5.34), 1.75 (95% CI = 1.23-2.50), and 1.58 (95% CI = 1.09-2.30), respectively. Participant mortality rate was 45% in the lowest quartile of UPSIT scores (anosmia) and 18% in the highest quartile of UPSIT scores.
Interpretation: Impaired odor identification, particularly in the anosmic range, is associated with increased mortality in older adults even after controlling for dementia and medical comorbidity.
© 2015 American Neurological Association.
Conflict of interest statement
D.P. Devanand has received consulting fees from AbbVie and Lundbeck. Richard Doty is President and major shareholder of Sensonics, Inc., a manufacturer and distributor of tests of taste and smell, including the UPSIT. Richard Doty has received publishing royalties from Cambridge University Press and Johns Hopkins University Press, and an honorarium from the University of Florida and lodging reimbursement as Chairperson of the Other Non-Motor Features of Parkinson’s Disease working group of the Parkinson Study Group. He has received consulting fees from Pfizer, Inc., Acorda Therapeutics and several law offices. There are no other conflicts of interest.
Figures

References
-
- Hyman BT, Arriagada PV, Van Hoesen GW. Pathologic changes in the olfactory system in aging and Alzheimer’s disease. Ann N Y Acad Sci. 1991;640:14–19. - PubMed
-
- Ross GW, Abbott RD, Petrovitch H, et al. Association of olfactory dysfunction with incidental Lewy bodies. Mov Disord. 2006;21:2062–2067. - PubMed
-
- Doty RL, Shaman P, Applebaum SL, et al. Smell identification ability: changes with age. Science. 1984;226:1441–1443. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
