

Efficiency of high-dose cytarabine added to CY/TBI in cord blood transplantation for myeloid malignancy
- PMID: 26031916
- PMCID: PMC4504951
- DOI: 10.1182/blood-2015-04-642652
Efficiency of high-dose cytarabine added to CY/TBI in cord blood transplantation for myeloid malignancy
Abstract
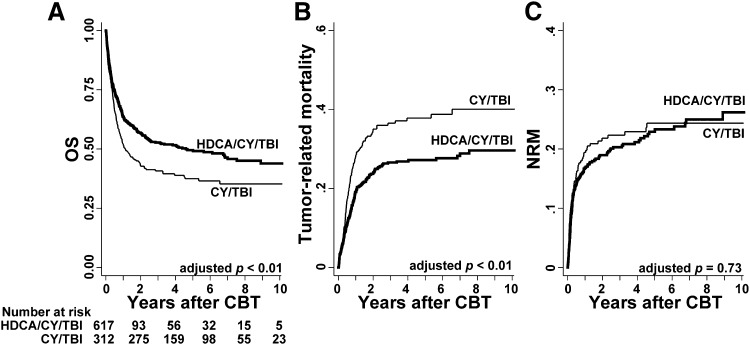
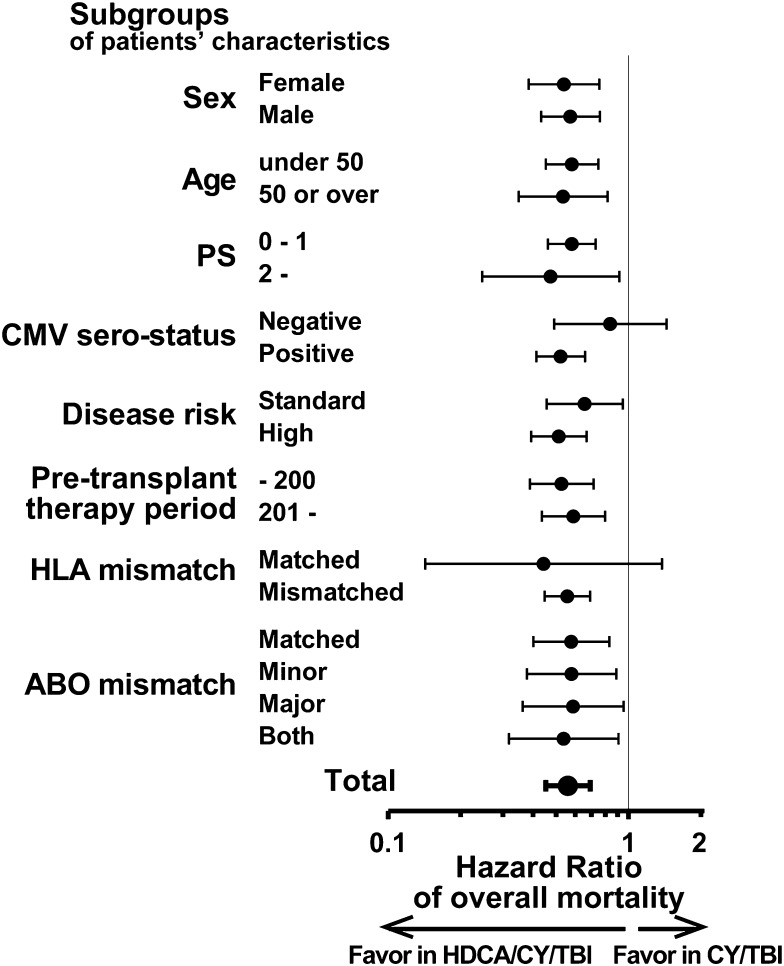
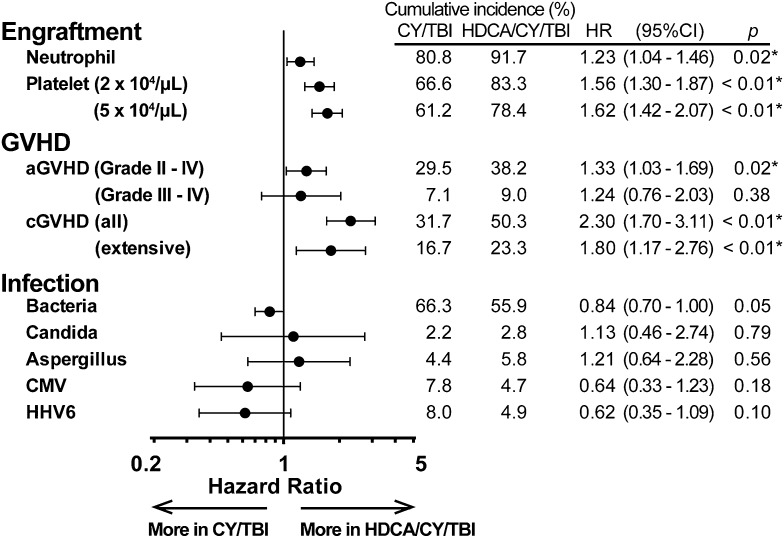
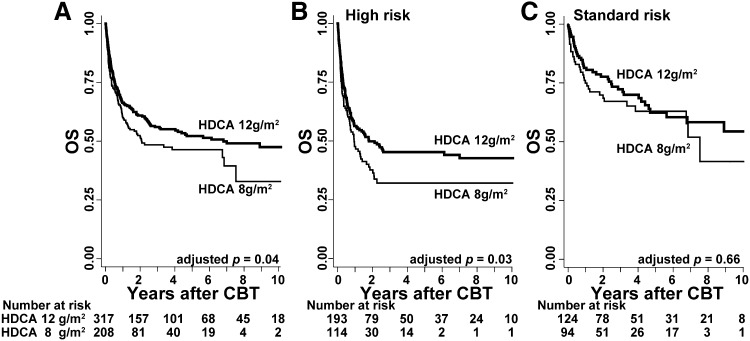
Cord blood transplantation (CBT) is an effective therapeutic option for adults with acute myelogenous leukemia (AML) and myelodysplastic syndrome (MDS) after the conventional cyclophosphamide and total body irradiation (CY/TBI) regimen, but posttransplant relapse is still of high importance. High-dose cytarabine (HDCA) can be added to CY/TBI for an intensified regimen; however, its additional effects have not yet been completely elucidated. Therefore, we conducted a cohort study to compare the prognosis of HDCA/CY/TBI (n = 617) and CY/TBI (n = 312) in CBT for AML/MDS, using a Japanese transplant registry database. The median age was 40 years, and 86.2% of the patients had AML; high-risk disease was observed in 56.2% of the patients. The median follow-up period after CBT was approximately 3.5 years. Overall survival was significantly superior in the HDCA/CY/TBI group (adjusted hazard ratio [HR], 0.56; 95% confidence interval [CI], 0.45-0.69; P < .01), and tumor-related mortality was lower (HR, 0.50; P < .01). The incidence of grade II to IV acute graft-vs-host disease (aGVHD) and chronic GVHD was significantly higher in the HDCA/CY/TBI group (HR, 1.33 and 2.30, respectively), but not grade III to IV aGVHD. Incidence of infectious episodes showed no significant difference. Nonrelapse mortality was not increased by the addition of HDCA. Higher-dose CA (12 rather than 8 g/m(2)) was more effective, particularly in patients at high-risk for disease. This study is the first to show the superiority of HDCA/CY/TBI to CY/TBI in CBT for AML/MDS. A large-scale prospective study is warranted to establish new conditioning regimens including HDCA administration.
© 2015 by The American Society of Hematology.
Figures
References
-
- Takahashi S, Ooi J, Tomonari A, et al. Comparative single-institute analysis of cord blood transplantation from unrelated donors with bone marrow or peripheral blood stem-cell transplants from related donors in adult patients with hematologic malignancies after myeloablative conditioning regimen. Blood. 2007;109(3):1322–1330. - PubMed
-
- Atsuta Y, Kanda J, Takanashi M, et al. HLA Working Group of the Japan Society for Hematopoietic Cell Transplantation. Different effects of HLA disparity on transplant outcomes after single-unit cord blood transplantation between pediatric and adult patients with leukemia. Haematologica. 2013;98(5):814–822. - PMC - PubMed
-
- Nagler A, Rocha V, Labopin M, et al. Allogeneic hematopoietic stem-cell transplantation for acute myeloid leukemia in remission: comparison of intravenous busulfan plus cyclophosphamide (Cy) versus total-body irradiation plus Cy as conditioning regimen—a report from the acute leukemia working party of the European group for blood and marrow transplantation. J Clin Oncol. 2013;31(28):3549–3556. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
