

Preoperative testing before low-risk surgical procedures
- PMID: 26032314
- PMCID: PMC4527930
- DOI: 10.1503/cmaj.150174
Preoperative testing before low-risk surgical procedures
Abstract
Background: There is concern about increasing utilization of low-value health care services, including preoperative testing for low-risk surgical procedures. We investigated temporal trends, explanatory factors, and institutional and regional variation in the utilization of testing before low-risk procedures.
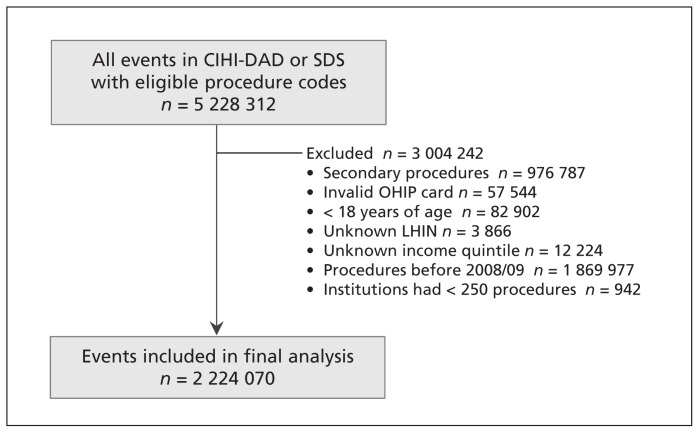
Methods: For this retrospective cohort study, we accessed linked population-based administrative databases from Ontario, Canada. A cohort of 1 546 223 patients 18 years or older underwent a total of 2 224 070 low-risk procedures, including endoscopy and ophthalmologic surgery, from Apr. 1, 2008, to Mar. 31, 2013, at 137 institutions in 14 health regions. We used hierarchical logistic regression models to assess patient- and institution-level factors associated with electrocardiography (ECG), transthoracic echocardiography, cardiac stress test or chest radiography within 60 days before the procedure.
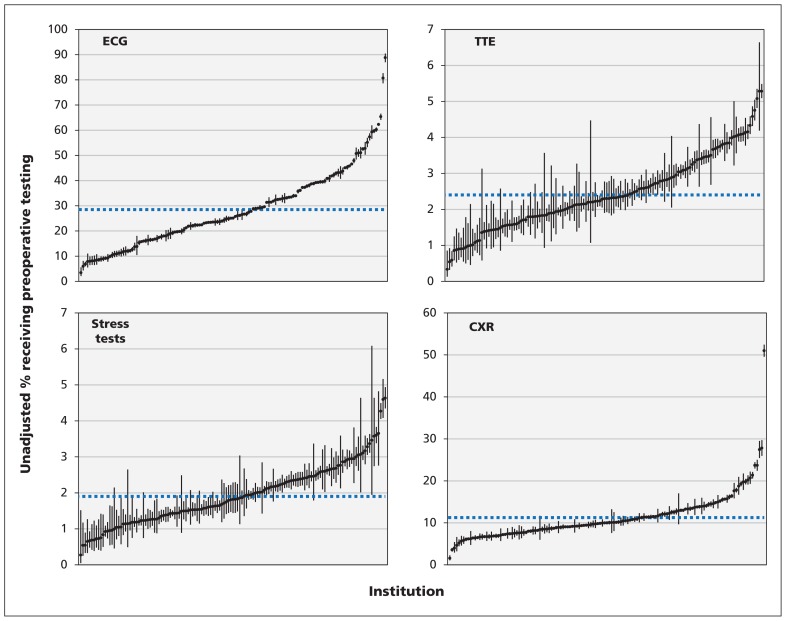
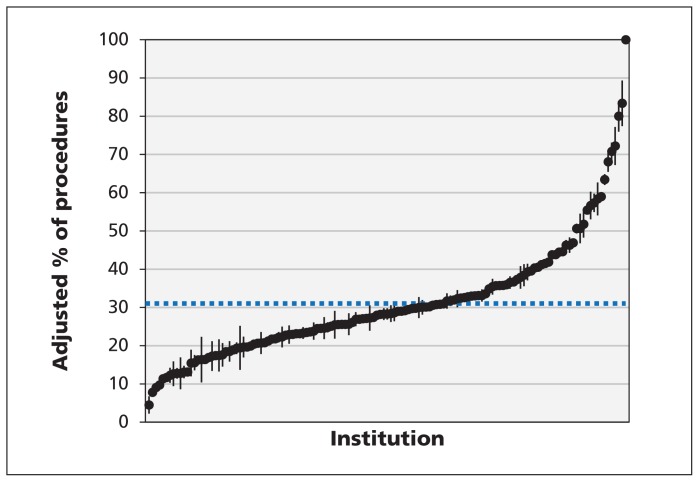
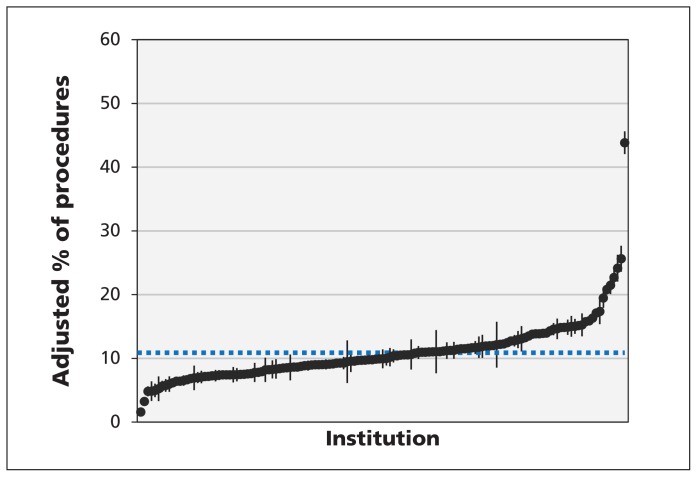
Results: Endoscopy, ophthalmologic surgery and other low-risk procedures accounted for 40.1%, 34.2% and 25.7% of procedures, respectively. ECG and chest radiography were conducted before 31.0% (95% confidence interval [CI] 30.9%-31.1%) and 10.8% (95% CI 10.8%-10.8%) of procedures, respectively, whereas the rates of preoperative echocardiography and stress testing were 2.9% (95% CI 2.9%-2.9%) and 2.1% (95% CI 2.1%-2.1%), respectively. Significant variation was present across institutions, with the frequency of preoperative ECG ranging from 3.4% to 88.8%. Receipt of preoperative ECG and radiography were associated with older age (among patients 66-75 years of age, for ECG, adjusted odds ratio [OR] 18.3, 95% CI 17.6-19.0; for radiography, adjusted OR 2.9, 95% CI 2.8-3.0), preoperative anesthesia consultation (for ECG, adjusted OR 8.7, 95% CI 8.5-8.8; for radiography, adjusted OR 2.2, 95% CI 2.1-2.2) and preoperative medical consultation (for ECG, adjusted OR 6.8, 95% CI 6.7-6.9; for radiography, adjusted OR 3.6, 95% CI 3.5-3.6). The median ORs for receipt of preoperative ECG and radiography were 2.3 and 1.6, respectively.
Interpretation: Despite guideline recommendations to limit testing before low-risk surgical procedures, preoperative ECG and chest radiography were performed frequently. Significant variation across institutions remained after adjustment for patient- and institution-level factors.
© 2015 Canadian Medical Association or its licensors.
Figures
References
-
- Cassel CK, Guest JA. Choosing wisely: helping physicians and patients make smart decisions about their care. JAMA 2012;307: 1801–2. - PubMed
-
- Levinson W, Kallewaard M, Bhatia RS, et al. ‘Choosing Wisely’: a growing international campaign. BMJ Qual Saf 2015; 24:167–74. - PubMed
-
- Canadian Cardiovascular Society. Cardiology: five things physicians and patients should question. Choosing Wisely Canada; 2014. Available: www.choosingwiselycanada.org/recommendations/cardiology/ (accessed 2015 May 14).
-
- Canadian Association of General Surgeons. Six things physicians and patients should question. Choosing Wisely Canada; 2014. Available: www.choosingwiselycanada.org/recommendations/general-surgery/ (accessed 2015 May 14).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous