

Examining the Impact of Separate Components of a Multicomponent Intervention Designed to Reduce At-Risk Drinking Among Older Adults: The Project SHARE Study
- PMID: 26033430
- PMCID: PMC4631261
- DOI: 10.1111/acer.12754
Examining the Impact of Separate Components of a Multicomponent Intervention Designed to Reduce At-Risk Drinking Among Older Adults: The Project SHARE Study
Abstract
Background: Health promotion interventions often include multiple components and several patient contacts. The objective of this study was to examine how participation within a multicomponent intervention (Project SHARE) is associated with changes in at-risk drinking among older adults.
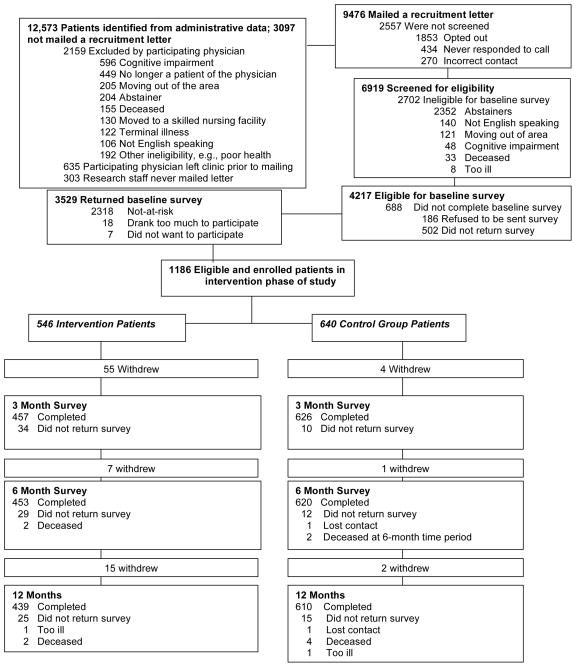
Methods: We analyzed observational data from a cluster-randomized trial of 31 primary care physicians and their patients aged ≥60 years, at a community-based practice with 7 clinics. Recruitment occurred between 2005 and 2007. At-risk drinkers in a particular physician's practice were randomly assigned as a group to usual care (n = 640 patients) versus intervention (n = 546 patients). The intervention included personalized reports, educational materials, drinking diaries, in-person physician advice, and telephone counseling by health educators (HEs). The primary outcome was at-risk drinking at follow-up, defined by scores on the Comorbidity Alcohol Risk Evaluation Tool (CARET). Predictors included whether a physician-patient alcohol risk discussion occurred, HE call occurred, drinking agreement with the HE was made, and patients self-reported keeping a drinking diary as suggested by the HE.
Results: At 6 months, there was no association of at-risk drinking with having had a physician-patient discussion. Compared to having had no HE call, the odds of at-risk drinking at 6 months were lower if an agreement was made or patients reported keeping a diary (odds ratio [OR] 0.58, 95% confidence interval [CI] 0.37 to 0.90), or if an agreement was made and patients reported keeping a diary (OR 0.52, CI 0.28 to 0.97). At 12 months, a physician-patient discussion (OR 0.61, CI 0.38 to 0.98) or an agreement and reported use of a diary (OR 0.45, CI 0.25) were associated with lower odds of at-risk drinking.
Conclusions: Within the Project SHARE intervention, discussing alcohol risk with a physician, making a drinking agreement, and/or self-reporting the use of a drinking diary were associated with lower odds of at-risk drinking at follow-up. Future studies targeting at-risk drinking among older adults should consider incorporating both intervention components.
Keywords: Alcohol Use; Drinking Agreement; Drinking Diary; Older Adults; Physician-Patient Discussion.
Copyright © 2015 by the Research Society on Alcoholism.
References
-
- Aira M, Kauhanen J, Larivaara P, Rautio P. Factors influencing inquiry about patients’ alcohol consumption by primary health care physicians: Qualitative semi-structured interview study. Fam Pract. 2003;20:270–275. - PubMed
-
- Byles J, Young A, Furuya H, Parkinson L. A drink to healthy aging: The association between older women’s use of alcohol and their health-related quality of life. J Am Geriatr Soc. 2006;54:1341–1347. - PubMed
-
- Carvalho ML, Honeycutt S, Escoffery C, Glanz K, Sabbs D, Kegler MC. Balancing fidelity and adaptation: implementing evidence-based chronic disease prevention programs. J Public Health Manag Pract. 2013;4:348–356. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
