

How are spousal depressed mood, distress, and quality of life associated with risk of depressed mood in cancer survivors? Longitudinal findings from a national sample
- PMID: 26033755
- PMCID: PMC4453017
- DOI: 10.1158/1055-9965.EPI-14-1420
How are spousal depressed mood, distress, and quality of life associated with risk of depressed mood in cancer survivors? Longitudinal findings from a national sample
Abstract
Background: Spouses of cancer survivors experience both positive and negative effects from caregiving. However, it is less clear what role spousal well-being may have on cancer survivors. This study aimed to determine the impact of spousal psychosocial factors on survivor depressed mood and whether this association differed by gender.
Methods: We examined longitudinal data on cancer survivors and their spouses (n = 910 dyads) from the 2004-2012 Medical Expenditures Panel Survey and a matched sample of cancer-free dyads. Subjects reported depressed mood, psychologic distress, and mental and physical health-related quality of life (HRQoL) at two time points (T1/T2). Dyadic multilevel models evaluated the impact of psychosocial factors at T1 on depressed mood at T2, controlling for sociodemographics, cancer type, survivor treatment status, and depressed mood at T1.
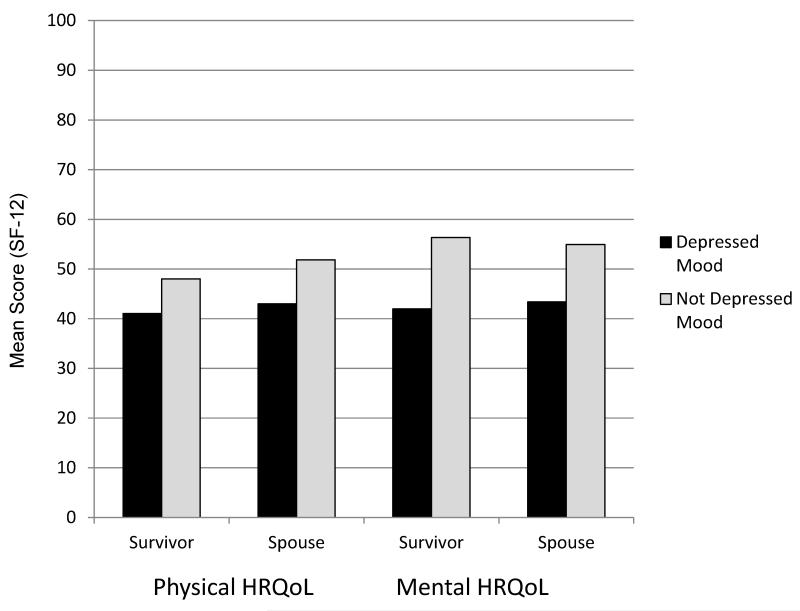
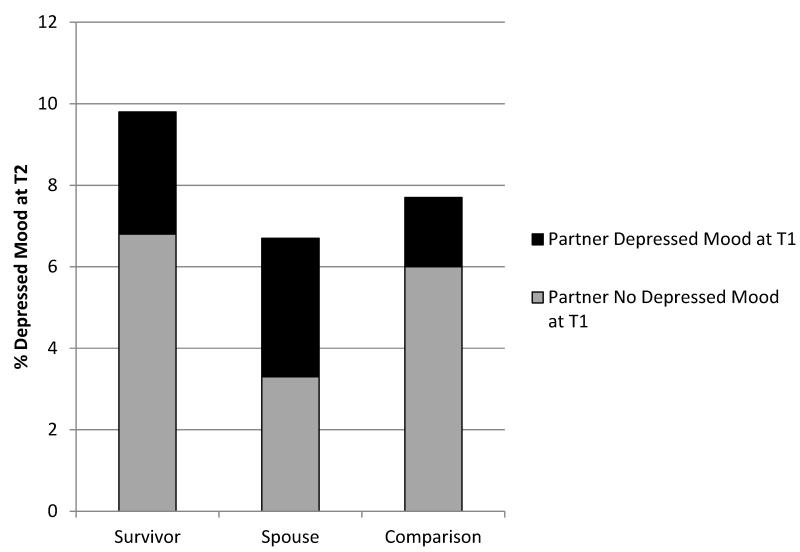
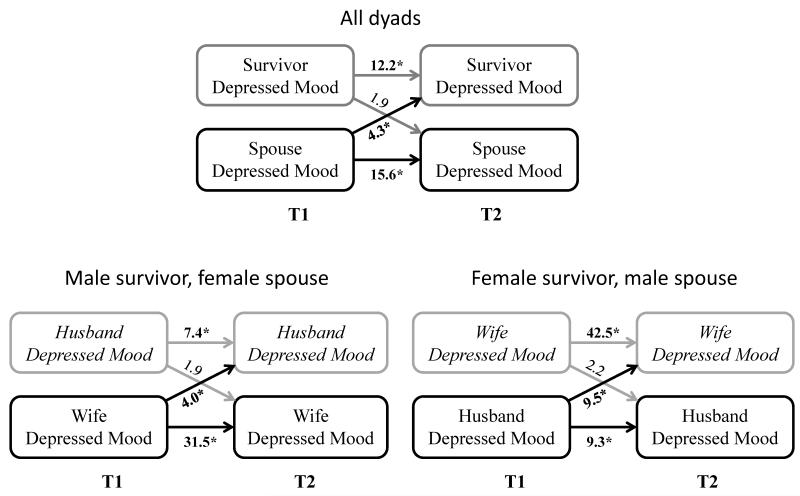
Results: Cancer survivors whose spouses reported depressed mood at T1 were 4.27 times more likely to report depressed mood at T2 [95% confidence interval (CI), 2.01-9.07]; this was stronger for female survivors (OR, 9.49; 95% CI, 2.42-37.20). Better spousal mental and physical HRQoL at T1 were associated with a 30% decrease in survivor depressed mood risk at T2. Most spillover effects were not observed in comparison dyads.
Conclusion: Depressed mood and poor HRQoL in spouses may increase the risk of depressed mood in cancer survivors. The risk may be especially strong for female survivors.
Impact: Identifying and improving spousal mental health and HRQoL problems may reduce the risk of depressed mood in cancer survivors. Future research should examine whether incorporating spousal care into psychooncology and survivorship programs improves survivor outcomes.
©2015 American Association for Cancer Research.
Figures
References
-
- Massie MJ. Prevalence of depression in patients with cancer. Journal of the National Cancer Institute Monographs. 2004:57–71. - PubMed
-
- Walker J, Holm Hansen C, Martin P, Sawhney A, Thekkumpurath P, Beale C, et al. Prevalence of depression in adults with cancer: a systematic review. Annals of oncology: official journal of the European Society for Medical Oncology/ESMO. 2013;24:895–900. - PubMed
-
- Dunn LB, Cooper BA, Neuhaus J, West C, Paul S, Aouizerat B, et al. Health psychology: official journal of the Division of Health Psychology. Vol. 30. American Psychological Association; 2011. Identification of distinct depressive symptom trajectories in women following surgery for breast cancer; pp. 683–92. - PMC - PubMed
-
- Helgeson VS, Snyder P, Seltman H. Health psychology: official journal of the Division of Health Psychology. Vol. 23. American Psychological Association; 2004. Psychological and physical adjustment to breast cancer over 4 years: identifying distinct trajectories of change; pp. 3–15. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
