

Role of Cardiac MR Imaging in Cardiomyopathies
- PMID: 26033902
- PMCID: PMC4465292
- DOI: 10.2967/jnumed.114.142729
Role of Cardiac MR Imaging in Cardiomyopathies
Abstract
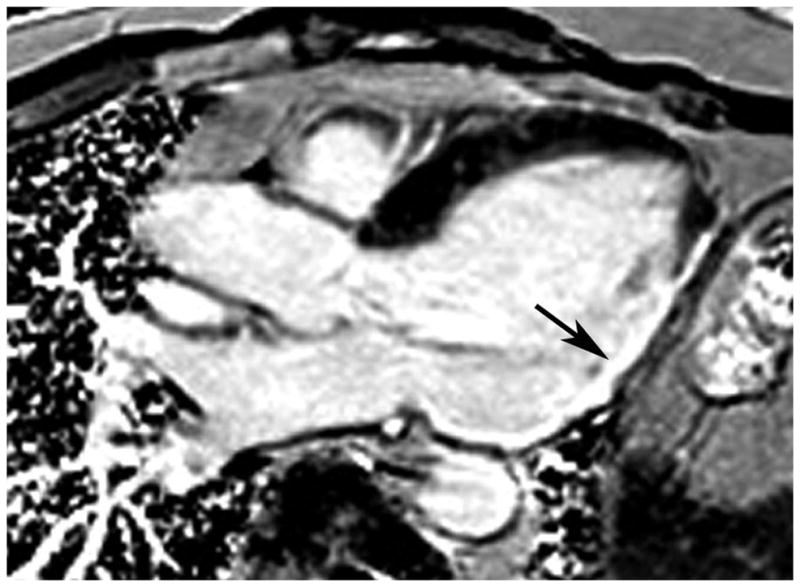
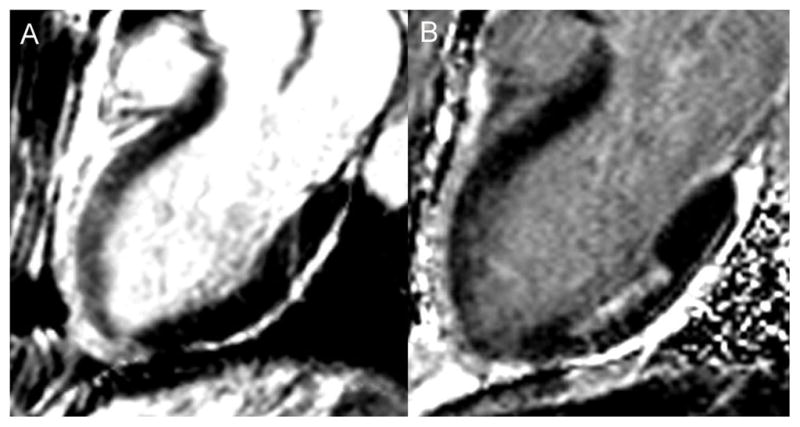
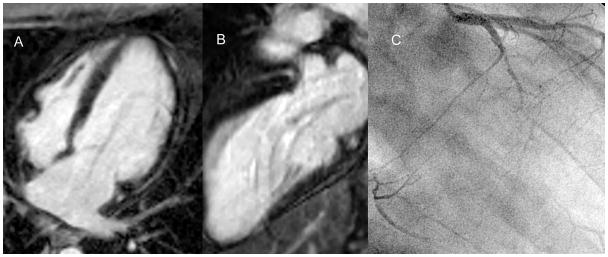
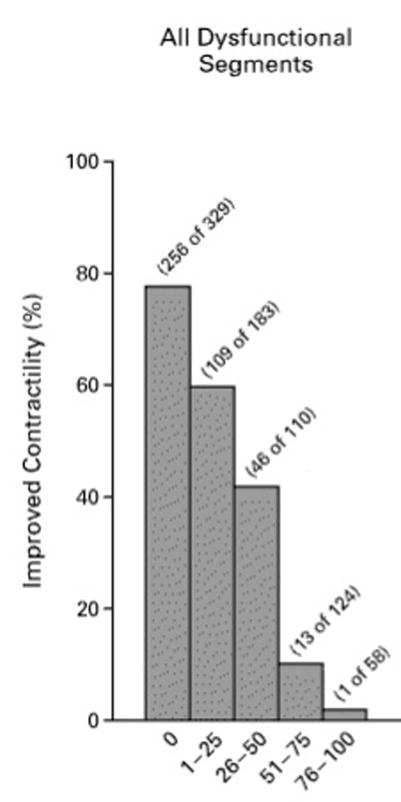
Cardiac MR imaging has made major inroads in the new millennium in the diagnosis and assessment of prognosis for patients with cardiomyopathies. Imaging of left and right ventricular structure and function and tissue characterization with late gadolinium enhancement (LGE) as well as T1 and T2 mapping enable accurate diagnosis of the underlying etiology. In the setting of coronary artery disease, either transmurality of LGE or contractile reserve in response to dobutamine can assess the likelihood of recovery of function after revascularization. The presence of scar reduces the likelihood of a response to medical therapy and to cardiac resynchronization therapy in heart failure. The presence and extent of LGE relate to overall cardiovascular outcome in cardiomyopathies. A major role for cardiac MR imaging in cardiomyopathies is to identify myocardial scar for diagnostic and prognostic purposes.
Keywords: cardiac MR imaging; coronary artery disease; infiltrative cardiomyopathy; ischemic cardiomyopathy; late gadolinium enhancement; nonischemic cardiomyopathy.
© 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
Figures
References
-
- Miller S, Simonetti OP, Carr J, Kramer U, Finn JP. MR imaging of the heart with cine true fast imaging with steady-state precession: influence of spatial and temporal resolutions on left ventricular functional parameters. Radiology. 2002;223:263–269. - PubMed
-
- Isbell DC, Kramer CM. Cardiovascular magnetic resonance: structure, function, perfusion, and viability. J Nucl Cardiol. 2005;12:324–336. - PubMed
-
- Grothues F, Smith GC, Moon JCC, et al. Comparison of interstudy reproducibility of cardiovascular magnetic resonance with two-dimensional echocardiography in normal subjects and in patients with heart failure or left ventricular hypertrophy. Am J Cardiol. 2002;90:29–34. - PubMed
-
- Bellenger NG, Davies LC, Francis JM, Coats AJS, Pennell DJ. Reduction in sample size for studies of remodeling in heart failure by the use of cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2000;2:271–278. - PubMed
-
- Zerhouni EA, Parish DM, Rogers WJ, Yang A, Shapiro EP. Human heart: tagging with MR imaging: a new method for noninvasive assessment of myocardial motion. Radiology. 1988;169:59–63. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical