

Changes in pulse pressure during hemodialysis treatment and survival in maintenance dialysis patients
- PMID: 26034226
- PMCID: PMC4491293
- DOI: 10.2215/CJN.09000914
Changes in pulse pressure during hemodialysis treatment and survival in maintenance dialysis patients
Abstract
Background and objectives: Pulse pressure has been shown as a risk factor for mortality in patients on maintenance hemodialysis (MHD). However, the effect of change in pulse pressure during hemodialysis on survival in a large cohort of patients on MHD has not been sufficiently investigated.
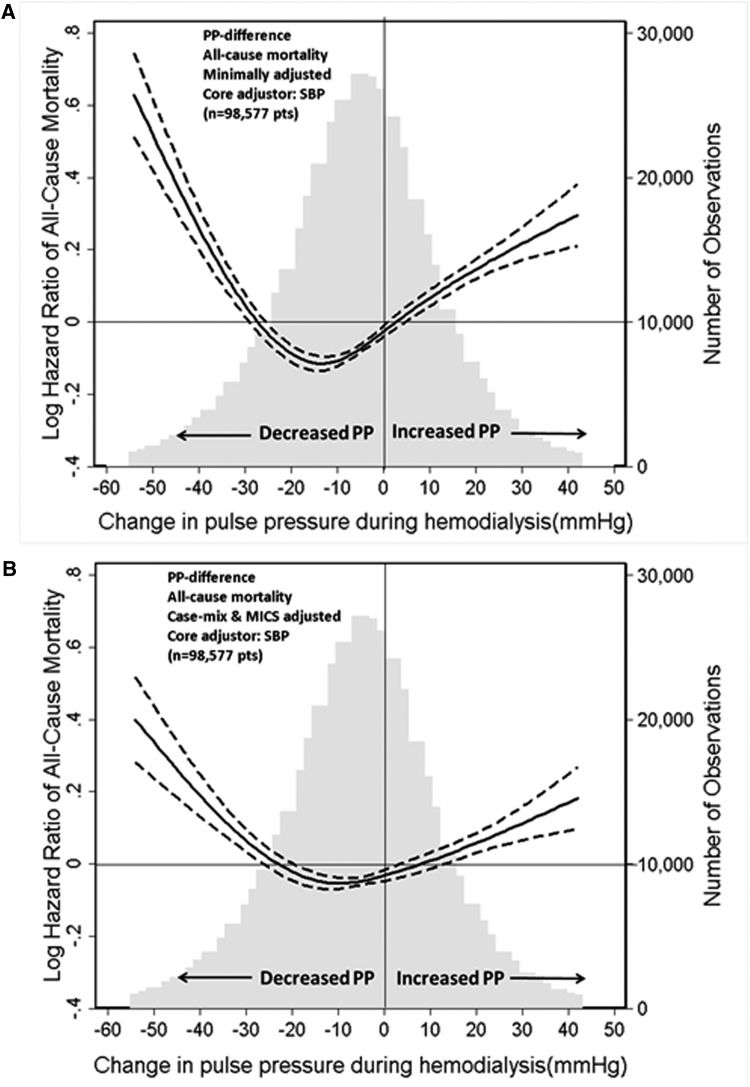
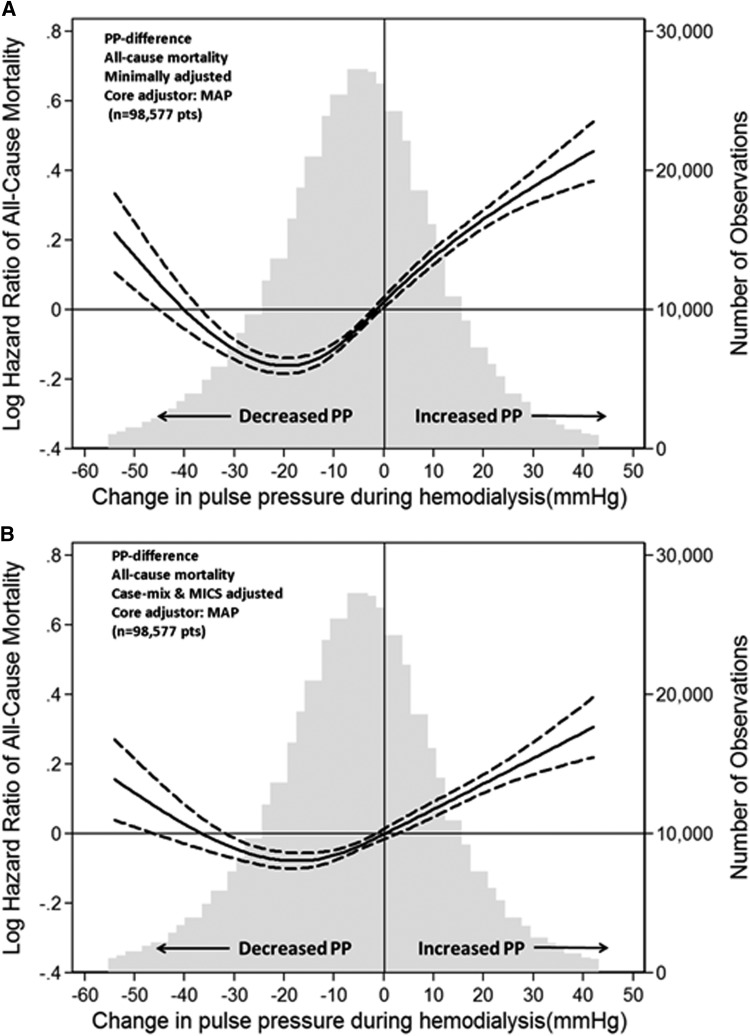
Design, setting, participants, & measurements: This study examined the association between time-varying Δ pulse pressure (postdialysis minus predialysis pulse pressure) and mortality in a cohort of 98,577 patients on MHD (July 2001-June 2006) using Cox proportional hazard models with restricted cubic splines.
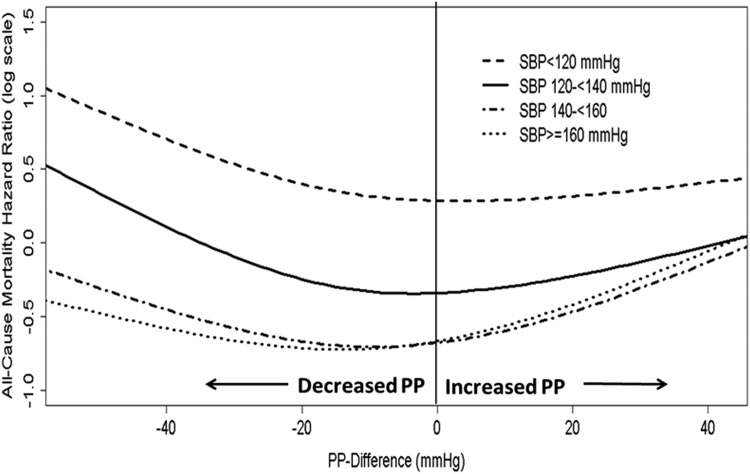
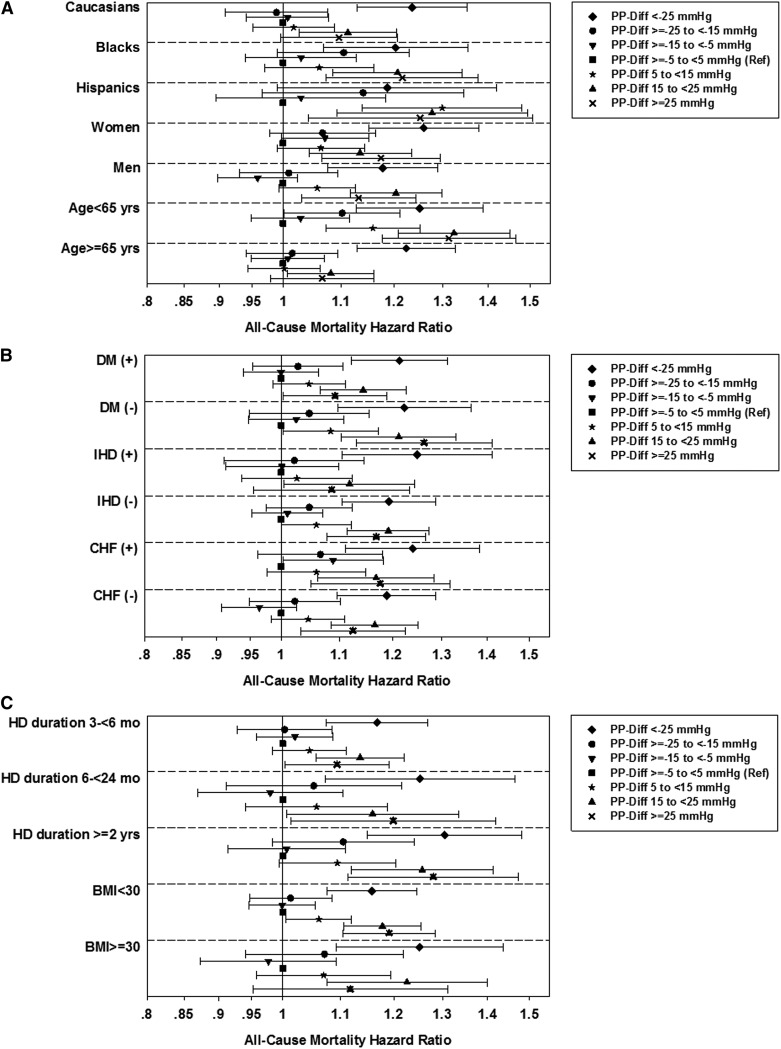
Results: The average patient age was 62 years old; among the patients, 33% were black and 59% had diabetes. During 134,814 patient-years of at-risk time, 16,054 (16%) patients died, with 6827 (43%) of the deaths caused by cardiovascular causes. In the models including adjustment for either predialysis systolic BP or mean arterial BP, there was a U-shaped association between change in pulse pressure during hemodialysis and all-cause mortality. In the systolic BP plus case mix plus malnutrition-inflammation complex syndrome-adjusted model, large declines in pulse pressure (>-25 mmHg) and increases in pulse pressure >5 mmHg were associated with higher all-cause mortality (reference: ≥-5 to <5 mmHg): hazard ratios (95% confidence intervals [95% CIs]) for change pulse pressures of <-25, ≥-25 to <-15, ≥-15 to <-5, 5 to <15, 15 to <25, and ≥25 mmHg were 1.21 (95% CI, 1.14 to 1.29), 1.03 (95% CI, 0.97 to 1.10), 1.01 (95% CI, 0.96 to 1.06), 1.06 (95% CI, 1.01 to 1.11), 1.17 (95% CI, 1.11 to 1.24), and 1.15 (95% CI, 1.08 to 1.23), respectively. The U-shaped association was observed with cardiovascular death.
Conclusions: Modest reductions in pulse pressure after hemodialysis are associated with the greatest survival, whereas large declines or rises in pulse pressure are related to higher mortality. Trials determining how to modify pulse pressure response to improve survival in the hemodialysis population are indicated.
Keywords: hemodialysis; hemodynamics and vascular regulation; survival.
Copyright © 2015 by the American Society of Nephrology.
Figures
References
-
- Benetos A, Rudnichi A, Safar M, Guize L: Pulse pressure and cardiovascular mortality in normotensive and hypertensive subjects. Hypertension 32: 560–564, 1998 - PubMed
-
- Domanski M, Norman J, Wolz M, Mitchell G, Pfeffer M: Cardiovascular risk assessment using pulse pressure in the first national health and nutrition examination survey (NHANES I). Hypertension 38: 793–797, 2001 - PubMed
-
- Franklin SS, Khan SA, Wong ND, Larson MG, Levy D: Is pulse pressure useful in predicting risk for coronary heart Disease? The Framingham heart study. Circulation 100: 354–360, 1999 - PubMed
-
- Millar JA, Lever AF, Burke V: Pulse pressure as a risk factor for cardiovascular events in the MRC Mild Hypertension Trial. J Hypertens 17: 1065–1072, 1999 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
