

Medical-Legal Strategies to Improve Infant Health Care: A Randomized Trial
- PMID: 26034248
- PMCID: PMC9923600
- DOI: 10.1542/peds.2014-2955
Medical-Legal Strategies to Improve Infant Health Care: A Randomized Trial
Abstract
Background: Changes in health care delivery create opportunities to improve systems to better meet the needs of low-income families while achieving quality benchmarks.
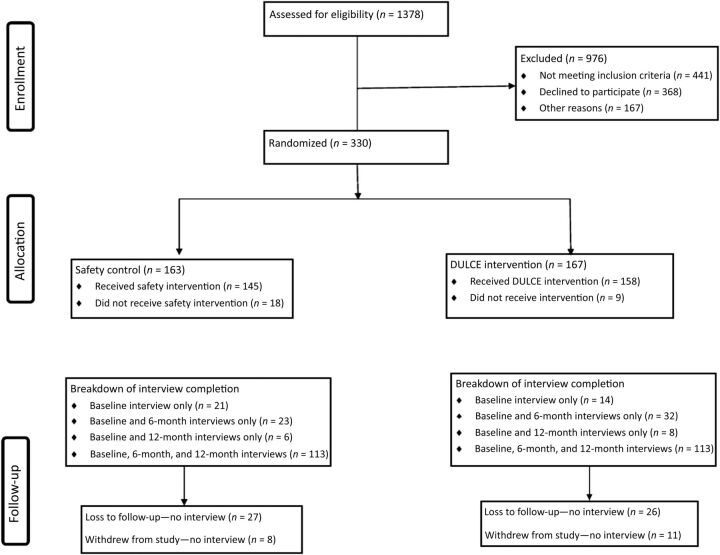
Methods: Families of healthy newborns receiving primary care at a single large urban safety-net hospital participated. Intervention families were randomly assigned a family specialist who provided support until the 6-month routine health care visit. The Developmental Understanding and Legal Collaboration for Everyone (DULCE) intervention is based on the Strengthening Families approach and incorporated components of the Healthy Steps and Medical-Legal Partnership models. Medical record reviews determined use of preventive and emergency care. Surveys conducted at baseline, postintervention (6 months), and follow-up (12 months) were used to determine hardship and attainment of concrete supports.
Results: Three hundred thirty families participated in the study. At baseline, 73% of families reported economic hardships. Intervention parents had an average of 14 contacts with the family specialist, and 5 hours of total contact time. Intervention infants were more likely to have completed their 6-month immunization schedule by age 7 months (77% vs 63%, P < .005) and by 8 months (88% vs 77%, P < .01). Intervention infants were more likely to have 5 or more routine preventive care visits by age 1 year (78% vs 67%, P < .01) and were less likely to have visited the emergency department by age 6 months (37% vs 49.7%, P < .03). The DULCE intervention accelerated access to concrete resources (P = .029).
Conclusions: Assignment to the Project DULCE intervention led to improvements in preventive health care delivery and utilization and accelerated access to concrete supports among low-income families.
Trial registration: ClinicalTrials.gov NCT01343940.
Copyright © 2015 by the American Academy of Pediatrics.
Conflict of interest statement
Figures

References
-
- Racine AD, Long TF, Helm ME, et al; Committee on Child Health Financing. Children’s Health Insurance Program (CHIP): accomplishments, challenges, and policy recommendations. Pediatrics. 2014;133(3). Available at: www.pediatrics.org/cgi/content/full/133/3/e784 - PubMed
-
- Mangione-Smith R , Schiff J , Dougherty D . Identifying children’s health care quality measures for Medicaid and CHIP: an evidence-informed, publicly transparent expert process. Acad Pediatr. 2011;11(suppl 3):S11–S21 - PubMed
-
- Urban Institute, Robert Wood Johnson Foundation. Gains for children: increased participation in Medicaid and CHIP in 2009. Available at: www.rwjf.org/content/dam/farm/reports/reports/2011/rwjf70806. Published 2011. Accessed March 25, 2014
-
- Conroy K , Sandel M , Zuckerman B . Poverty grown up: how childhood socioeconomic status impacts adult health. J Dev Behav Pediatr. 2010;31(2):154–160 - PubMed
