

Disaster nephrology: a new concept for an old problem
- PMID: 26034592
- PMCID: PMC4440471
- DOI: 10.1093/ckj/sfv024
Disaster nephrology: a new concept for an old problem
Abstract
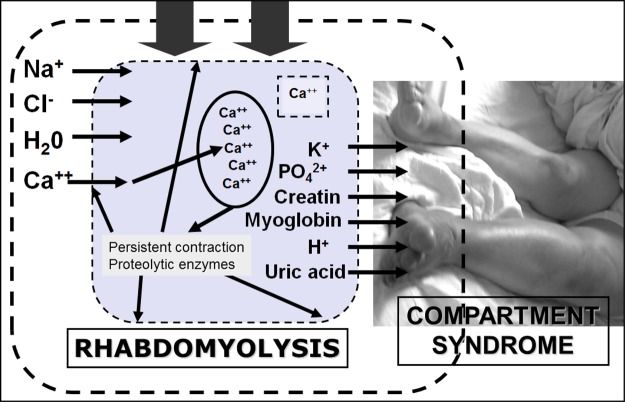
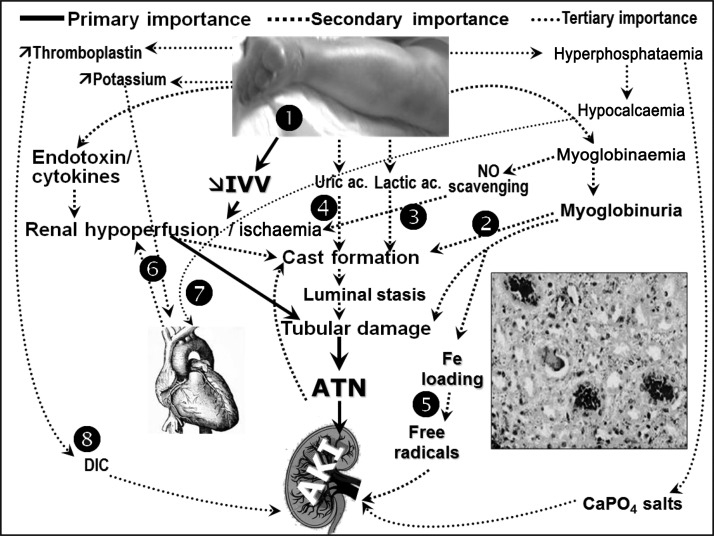
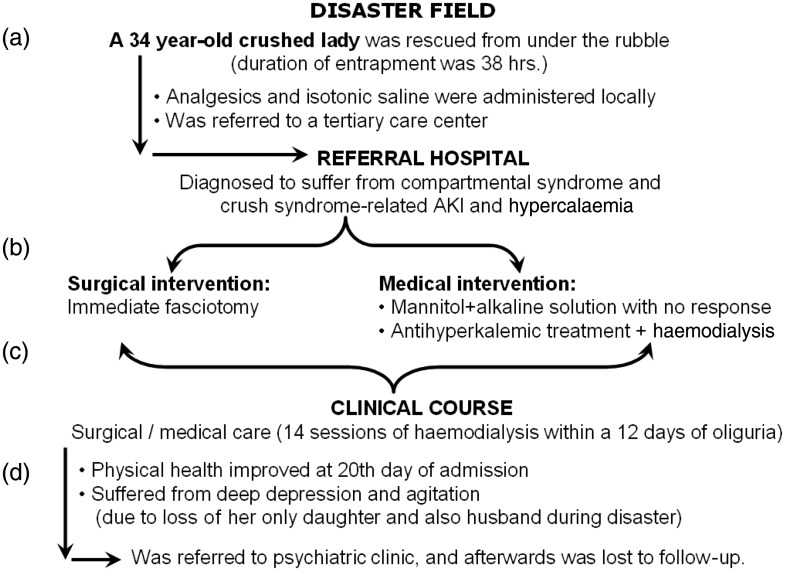
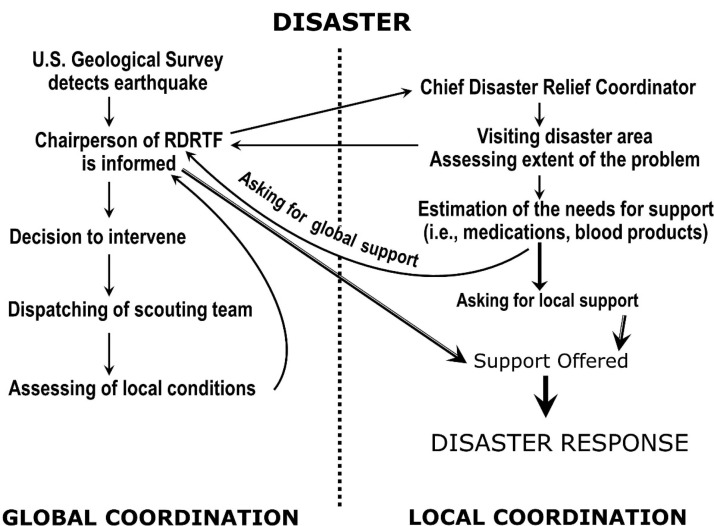
Natural and man-made mass disasters directly or indirectly affect huge populations, who need basic infrastructural help and support to survive. However, despite the potentially negative impact on survival chances, these health care issues are often neglected by the authorities. Treatment of both acute and chronic kidney diseases (CKDs) is especially problematic after disasters, because they almost always require complex technology and equipment, whereas specific drugs may be difficult to acquire for the treatment of the chronic kidney patients. Since many crush victims in spite of being rescued alive from under the rubble die afterward due to lack of dialysis possibilities, the terminology of 'renal disaster' was introduced after the Armenian earthquake. It should be remembered that apart from crush syndrome, multiple aetiologies of acute kidney injury (AKI) may be at play in disaster circumstances. The term 'seismonephrology' (or earthquake nephrology) was introduced to describe the need to treat not only a large number of AKI cases, but the management of patients with CKD not yet on renal replacement, as well as of patients on haemodialysis or peritoneal dialysis and transplanted patients. This wording was later replaced by 'disaster nephrology', because besides earthquakes, many other disasters such as hurricanes, tsunamis or wars may have a negative impact on the ultimate outcome of kidney patients. Disaster nephrology describes the handling of the many medical and logistic problems in treating kidney patients in difficult circumstances and also to avoid post-disaster chaos, which can be made possible by preparing medical and logistic scenarios. Learning and applying the basic principles of disaster nephrology is vital to minimize the risk of death both in AKI and CKD patients.
Keywords: AKI; acute tubular necrosis; chronic renal failure; dialysis; rhabdomyolysis.
Figures
References
-
- Gibney RT, Sever MS, Vanholder RC. Disaster nephrology: crush injury and beyond. Kidney Int 2014; 85: 1049–1057 - PubMed
-
- Reports of Statistics Institution of the Turkish Prime Ministry. Crisis Center of the Turkish Prime Ministry, Ankara, 1997, pp: 3–15.
-
- Slater MS, Mullins RJ. Rhabdomyolysis and myoglobinuric renal failure in trauma and surgical patients: a review. J Am Coll Surg 1998; 186: 693–716 - PubMed
-
- Bywaters EG, Beall D. Crush injuries with impairment of renal function. 1941. J Am Soc Nephrol 1998; 9: 322–332 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
