

Impact of Decentralized Care and the Xpert MTB/RIF Test on Rifampicin-Resistant Tuberculosis Treatment Initiation in Khayelitsha, South Africa
- PMID: 26034764
- PMCID: PMC4438894
- DOI: 10.1093/ofid/ofv014
Impact of Decentralized Care and the Xpert MTB/RIF Test on Rifampicin-Resistant Tuberculosis Treatment Initiation in Khayelitsha, South Africa
Abstract
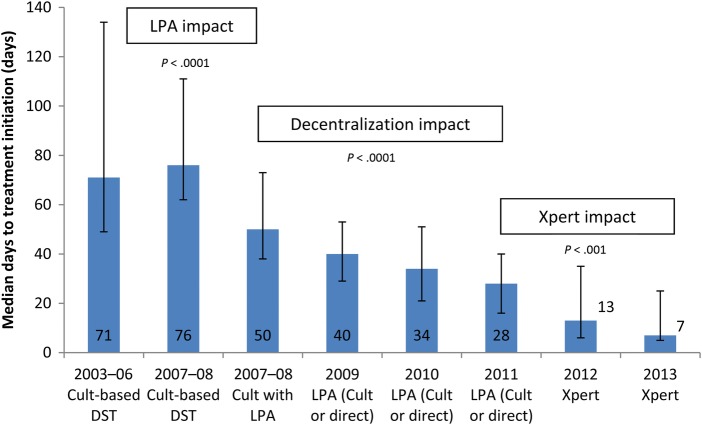
Background. Globally, case detection and treatment access are poor for rifampicin-resistant tuberculosis (RR-TB). The Xpert MTB/RIF test has the potential to increase detection and reduce time to treatment (TTT). However, these benefits are dependent on health system capacity to provide treatment. Methods. We retrospectively assessed the impact of Xpert on treatment initiation and TTT in the context of decentralized RR-TB care in Khayelitsha, Cape Town, using routine programmatic data. Community-based treatment was introduced progressively from 2008. Before 2007, diagnosis relied on phenotypic resistance (culture). During 2007-2008, the line probe assay (LPA) was introduced, followed by Xpert in 2012. Results. Before decentralization (2003-2006), median TTT was 71 days (interquartile range [IQR], 49-134; n = 158). The LPA introduction during 2007-2008 was associated with reduced median TTT from 76 to 50 days (P < .0001, n = 257). Between January 2009 and June 2013, 938 RR-TB cases were diagnosed (74% human immunodeficiency virus [HIV]-infected). Decentralization during 2008-2011 was associated with declining TTT (P < .0001, test for trend), a decline to 28 days in 2011 (IQR, 16-40; n = 173). Xpert was associated with a further reduction to 8 days in 2013 (IQR, 5-25; n = 89; P < .0001). Treatment initiation remained unchanged with Xpert and was lower among HIV-infected (2010-2013); 87.9% (445 of 506) compared with 96.9% (188 of 194) for HIV-uninfected (P < .0001) patients. Conclusions. Improved case detection and rapid treatment initiation are required to interrupt transmission and reduce mortality. In this setting, decentralization was associated with high treatment initiation and reduced TTT. Xpert implementation significantly enhanced the reduction in TTT and has the potential to reduce transmission.
Keywords: MDR-TB; RR-TB; Xpert; delay; treatment.
Figures
References
-
- Zhao Y, Xu S, Wang L, et al. National survey of drug-resistant tuberculosis in China. N Engl J Med. 2012;366:2161–70. - PubMed
-
- World Health Organization. Geneva: World Health Organization; 2014. Global Tuberculosis Report 2014.
-
- Gandhi NR, Shah NS, Andrews JR, et al. HIV coinfection in multidrug- and extensively drug-resistant tuberculosis results in high early mortality. Am J Respir Crit Care Med. 2010;181:80–6. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
