

Epidemiology of Kaposi's sarcoma-associated herpesvirus in HIV-1-infected US persons in the era of combination antiretroviral therapy
- PMID: 26035321
- PMCID: PMC6680245
- DOI: 10.1097/QAD.0000000000000682
Epidemiology of Kaposi's sarcoma-associated herpesvirus in HIV-1-infected US persons in the era of combination antiretroviral therapy
Abstract
Objective: To determine the effect of the introduction of combination antiretroviral treatment (cART) in the HIV-1-infected US population on the epidemiology of Kaposi's sarcoma-associated herpesvirus (KSHV).
Design, setting and participants: We investigated the epidemiology of KSHV in 5022 HIV-1-infected, antiretroviral-naive US persons participating in six AIDS Clinical Trials Group (ACTG)-randomized clinical trials, and followed in a long-term cohort study. We tested the first and last available sera of each participant for antibodies to KSHV K8.1 and ORF73.
Main outcome measures: We studied prevalence and incidence of KSHV infection, incidence of Kaposi's sarcoma, and overall survival.
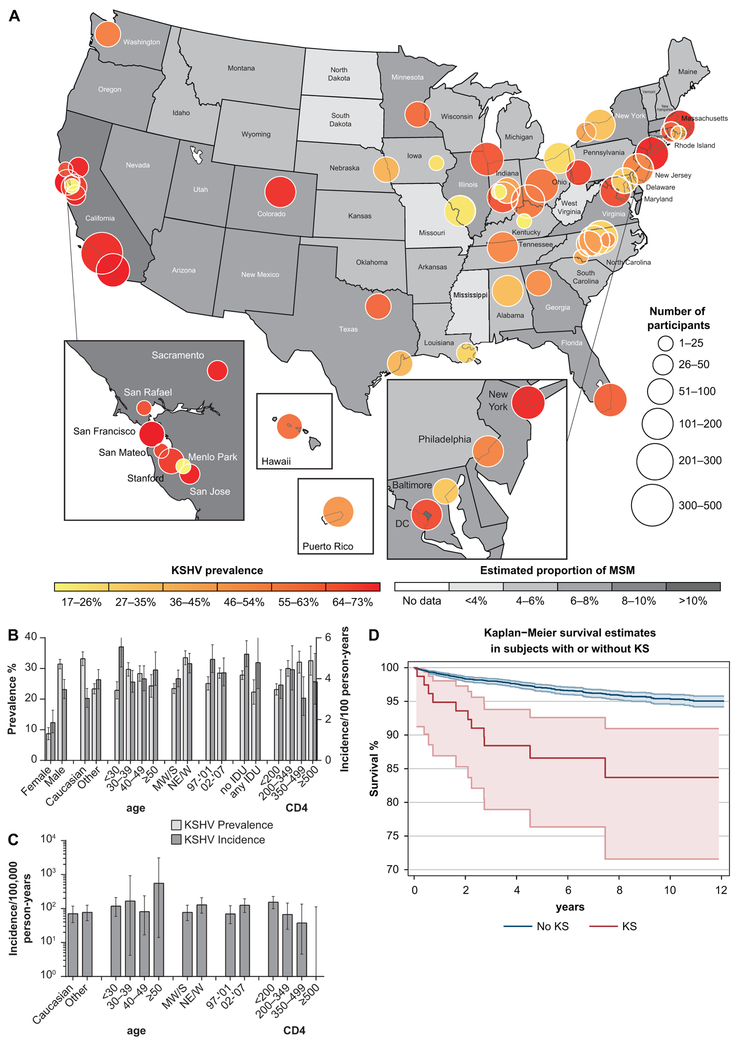
Results: KSHV prevalence was 38.1% [95% confidence interval (CI) 36.8-39.5%]. Male sex, Caucasian race, age between 30 and 49 years, residence in north-eastern or western United States, and enrolment after 2001 were independently associated with prevalent infection. KSHV incidence was 4.07/100 person-years (95% CI 3.70-4.47). Male sex, Caucasian race, age below 30, and enrolment after 2001 were associated with incident infection. CD4 cell count increase following cART was associated with lower risk. Kaposi's sarcoma incidence was 104.05/100 000 person-years (95% CI 71.17-146.89). Higher baseline CD4 cell count, but not increase in CD4 cell count after cART, was associated with lower hazard of Kaposi's sarcoma. Randomized assignment of protease inhibitors was not associated with better KSHV outcomes.
Conclusions: HIV-1-infected individuals, in particular Caucasian men, remain at a significant risk for KSHV co-infection and Kaposi's sarcoma. Thus, optimal management of HIV-1 infection should continue to include vigilance for manifestations of KSHV co-infection, including Kaposi's sarcoma.
Figures
References
-
- de Sanjose S, Mbisa G, Perez-Alvarez S, Benavente Y, Sukvirach S, Hieu NT, et al. Geographic Variation in the Prevalence of Kaposi Sarcoma-Associated Herpesvirus and Risk Factors for Transmission. J Infect Dis 2009,199:1449–1456. - PubMed
-
- Martin J The epidemiology of KSHV and its association with malignant disease In: Herpesviruses: Biology, Therapy, and Immunoprophylaxis. Cambridge: Cambridge University Press; 2007. Chapter 54. Edited by Arvin A GC-F, Mocarski E, Moore PS, Roizman B, Whitley R, Yamanishi K. Cambridge: Cambridge University Press; 2007.
-
- Martin JN, Ganem DE, Osmond DH, Page-Shafer KA, Macrae D, Kedes DH. Sexual transmission and the natural history of human herpesvirus 8 infection. N Engl J Med 1998,338:948–954. - PubMed
-
- Melbye M, Cook PM, Hjalgrim H, Begtrup K, Simpson GR, Biggar RJ, et al. Risk factors for Kaposi’s-sarcoma-associated herpesvirus (KSHV/HHV-8) seropositivity in a cohort of homosexual men, 1981–1996. Int J Cancer 1998,77:543–548. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
