

Fragility fractures of the sacrum: how to identify and when to treat surgically?
- PMID: 26038048
- PMCID: PMC4523697
- DOI: 10.1007/s00068-015-0530-z
Fragility fractures of the sacrum: how to identify and when to treat surgically?
Abstract
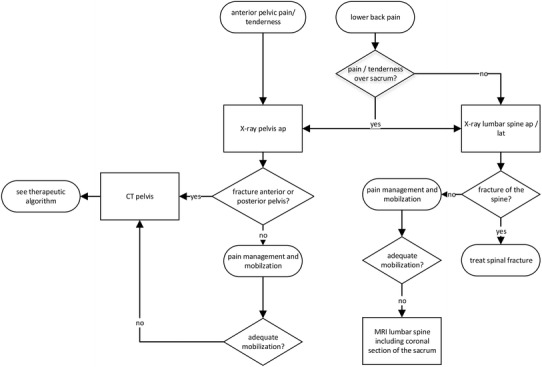
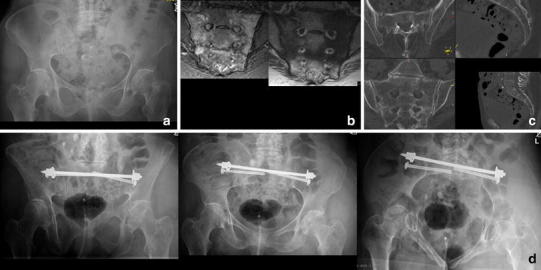
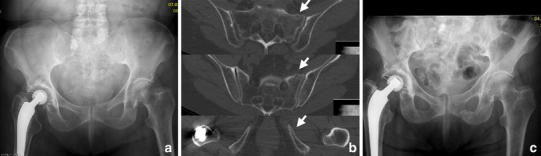
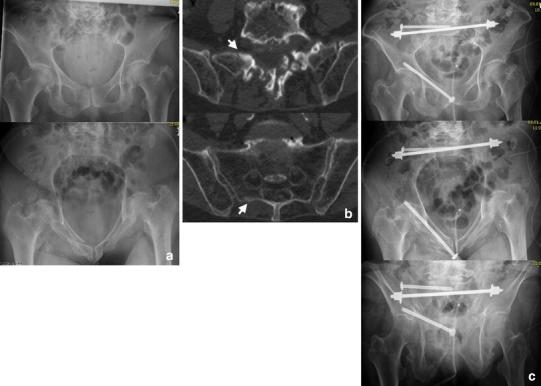
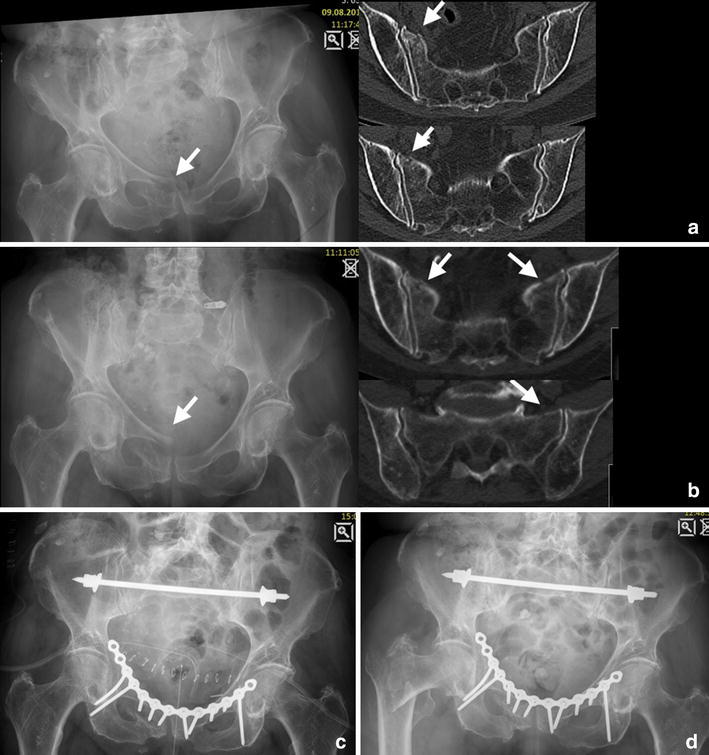
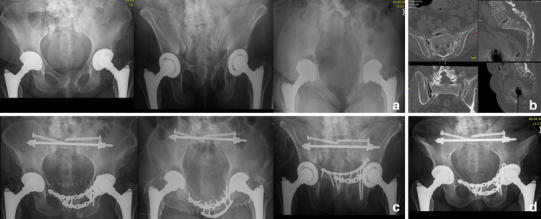
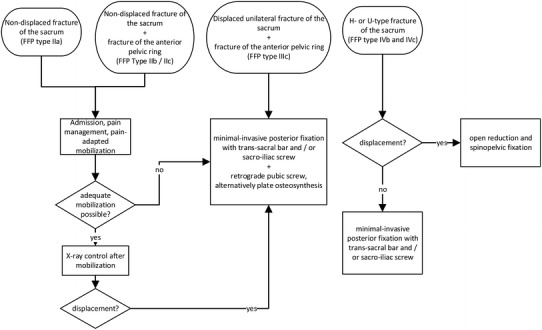
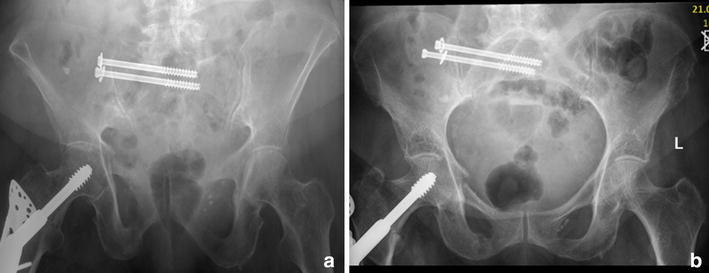
The increasing prevalence of fragility fractures of the sacrum (FFS) occurring predominantly in osteoporotic individuals poses a diagnostic and therapeutic challenge. The clinical presentation varies from longstanding low back pain without the patient remembering a traumatic event to immobilized patients after suffering a low-energy trauma. FFS are often combined with a fracture of the anterior pelvic ring; hence they are classified as a part of fragility fractures of the pelvis (FFP). If not displaced, the patients are treated with weight bearing as tolerated and analgesics; however, we advocate to treat displaced fractures surgically according to the fracture personality and the patient's comorbidities. Surgical options include minimal invasive sacro-iliac screws, trans-sacral bar osteosynthesis, open reduction and internal fixation, or spinopelvic stabilization. In the light of the high complication rate associated with immobilized patients, an operative approach often is indicated to accelerate the patient's mobility.
Figures
References
-
- Leidig-Bruckner G, Raue F, Frank-Raue K. Secondary osteoporosis—relevant clinical characteristics in diagnosis and therapy. Dtsch Med Wochenschr. 2012;137:326–332. - PubMed
-
- Consensus Development Conference Prophylaxis and treatment of osteoporosis. Am J Med. 1991;90:107–110. - PubMed
-
- Hernlund E, Svedbom A, Ivergård M, Compston J, Cooper C, Stenmark J, et al. Osteoporosis in the European Union: medical management, epidemiology and economic burden. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch. Osteoporos. 2013;8:136. - PMC - PubMed
-
- Kanis JA, Johnell O, Oden A, Jonsson B, De Laet C, Dawson A. Risk of hip fracture according to the World Health Organization criteria for osteopenia and osteoporosis. Bone. 2000;27:585–590. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
