

Iatrogenic hepatopancreaticobiliary injuries: a review
- PMID: 26038625
- PMCID: PMC4447885
- DOI: 10.1055/s-0035-1549377
Iatrogenic hepatopancreaticobiliary injuries: a review
Abstract
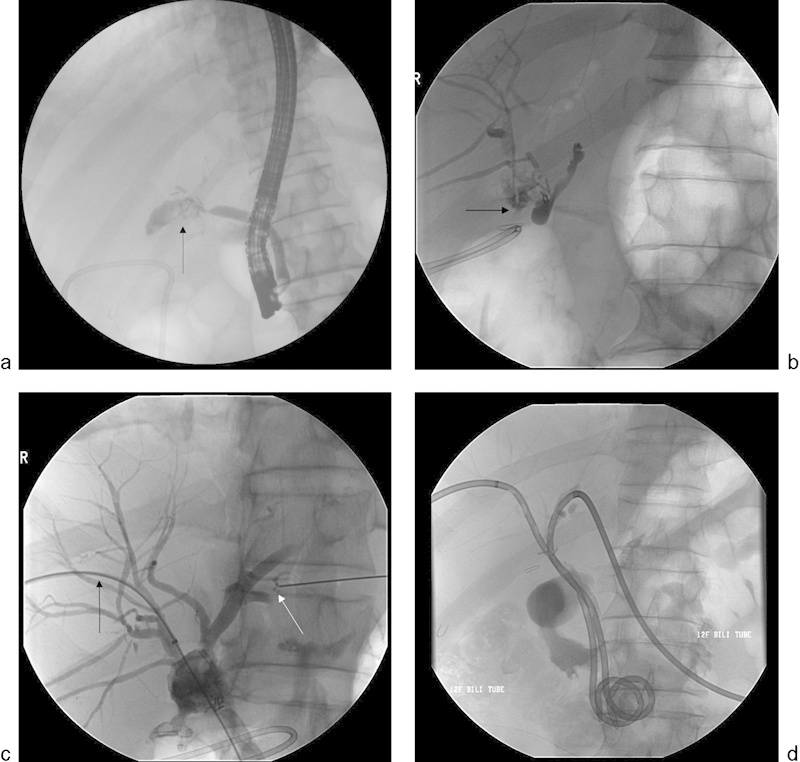
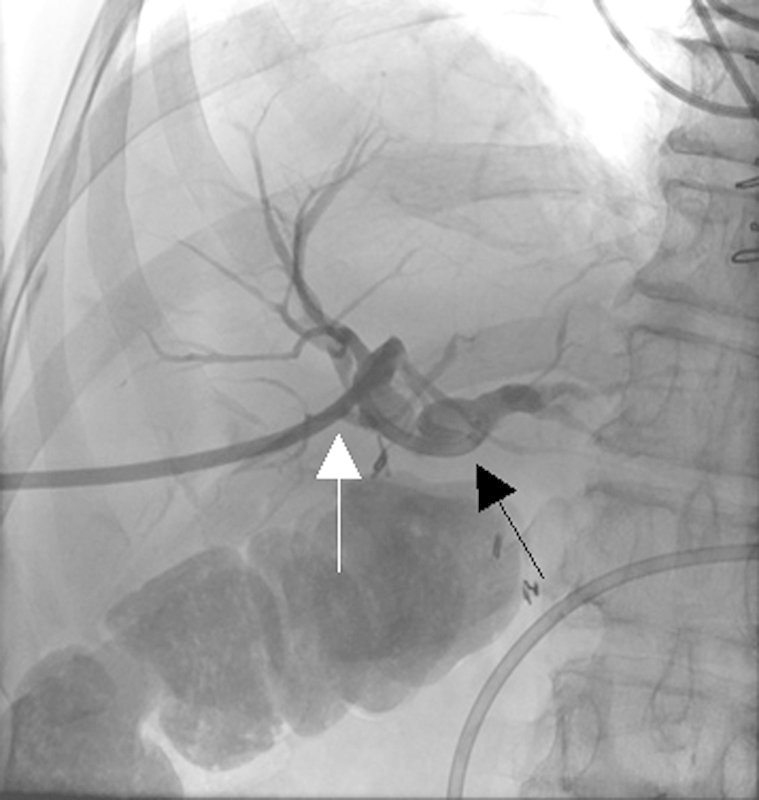
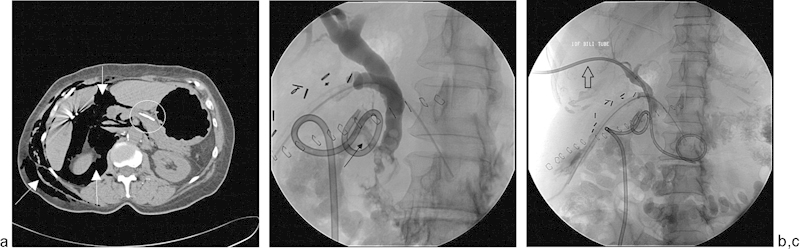
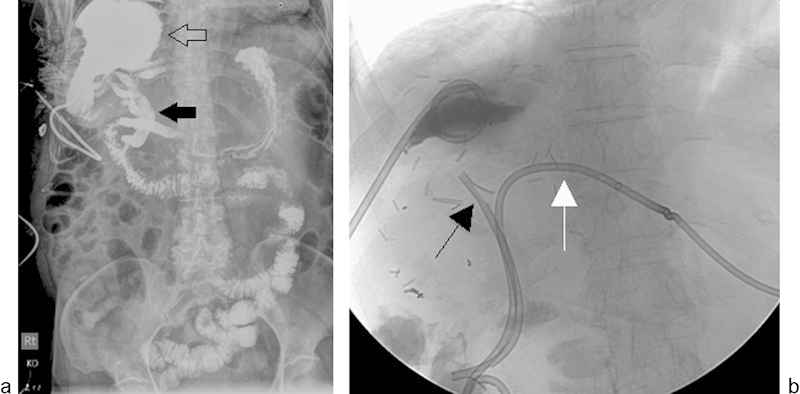
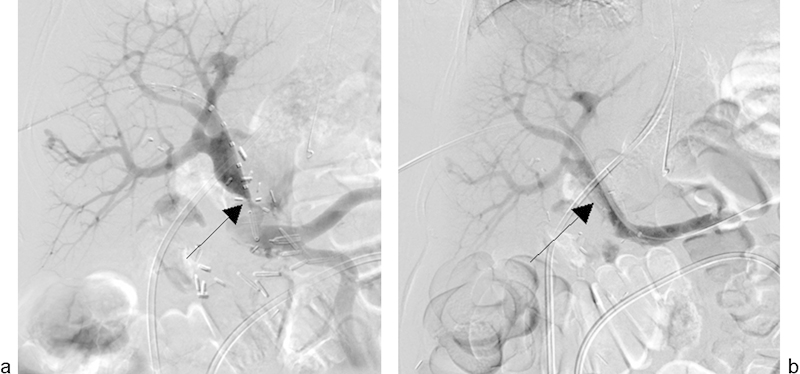
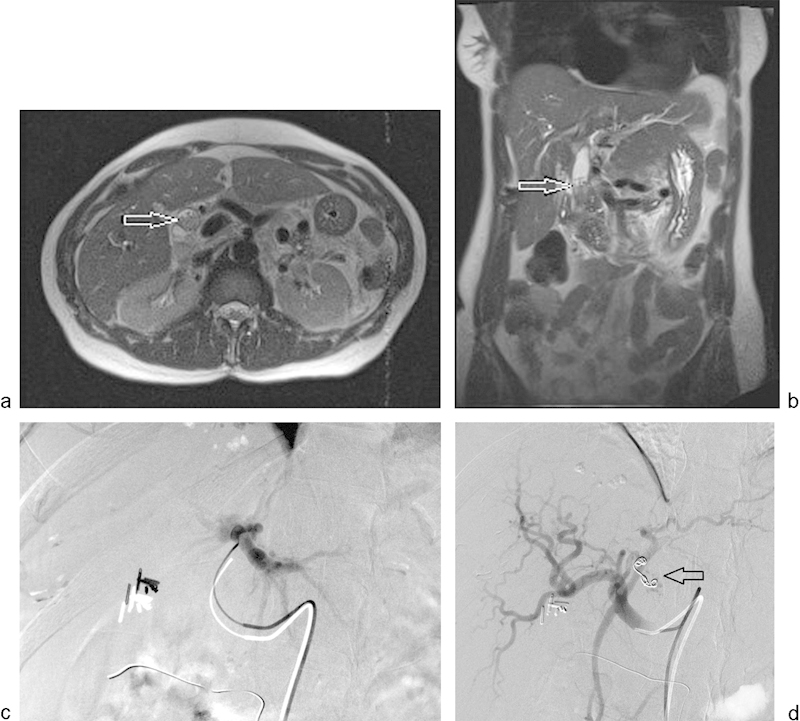
Iatrogenic hepatopancreaticobiliary injuries occur after various types of surgical and nonsurgical procedures. Symptomatically, these injuries may lead to a variety of clinical presentations, including tachycardia and hypotension from hemobilia or hemorrhage. Iatrogenic injuries may be identified during the intervention, immediately afterwards, or have a delayed presentation. These injuries are categorized into nonvascular and vascular injuries. Nonvascular injuries include biliary injuries such as biliary leak or stricture, pancreatic injury, and the development of fluid collections such as abscesses. Vascular injuries include pseudoaneurysms, arteriovenous fistulas, dissection, and perforation. Imaging studies such as ultrasound, computed tomography, magnetic resonance imaging, and digital subtraction angiography are critical for proper diagnosis of these conditions. In this article, we describe the clinical and imaging presentations of these iatrogenic injuries and the armamentarium of minimally invasive procedures (percutaneous drainage catheter placement, balloon dilatation, stenting, and coil embolization) that are useful in their management.
Keywords: bile duct injury; hepatobiliary; hepatopancreaticobiliary; iatrogenic injuries; interventional radiology.
Figures


References
-
- Lau W Y, Lai E C, Lau S H. Management of bile duct injury after laparoscopic cholecystectomy: a review. ANZ J Surg. 2010;80(1–2):75–81. - PubMed
-
- Nuzzo G, Giuliante F, Giovannini I. et al.Advantages of multidisciplinary management of bile duct injuries occurring during cholecystectomy. Am J Surg. 2008;195(6):763–769. - PubMed
-
- Flum D R, Cheadle A, Prela C, Dellinger E P, Chan L. Bile duct injury during cholecystectomy and survival in Medicare beneficiaries. JAMA. 2003;290(16):2168–2173. - PubMed
-
- Saad N, Darcy M. Iatrogenic bile duct injury during laparoscopic cholecystectomy. Tech Vasc Interv Radiol. 2008;11(2):102–110. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
