

Iatrogenic urinary tract injuries: etiology, diagnosis, and management
- PMID: 26038626
- PMCID: PMC4447880
- DOI: 10.1055/s-0035-1549378
Iatrogenic urinary tract injuries: etiology, diagnosis, and management
Abstract
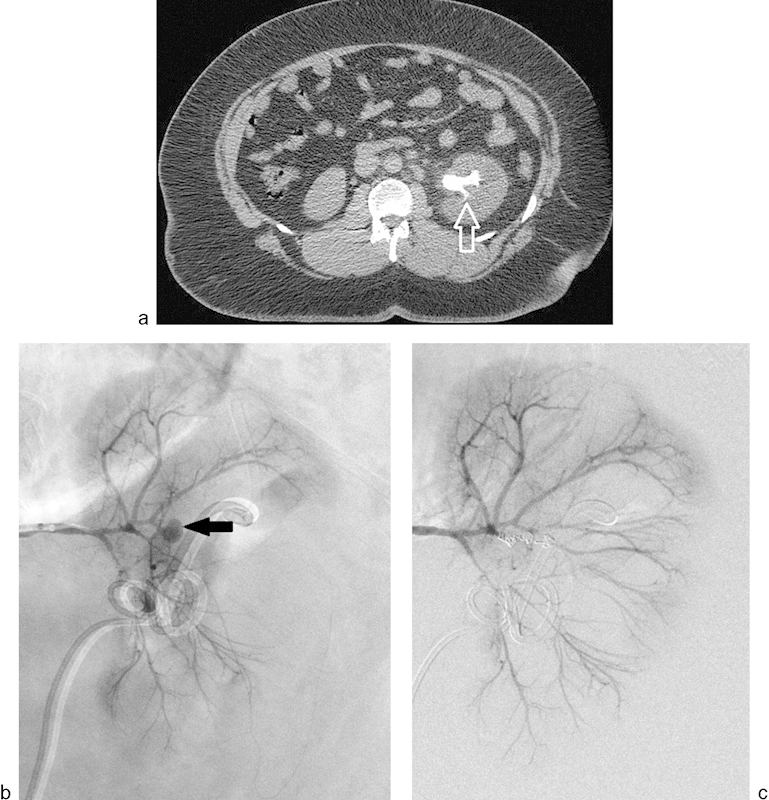
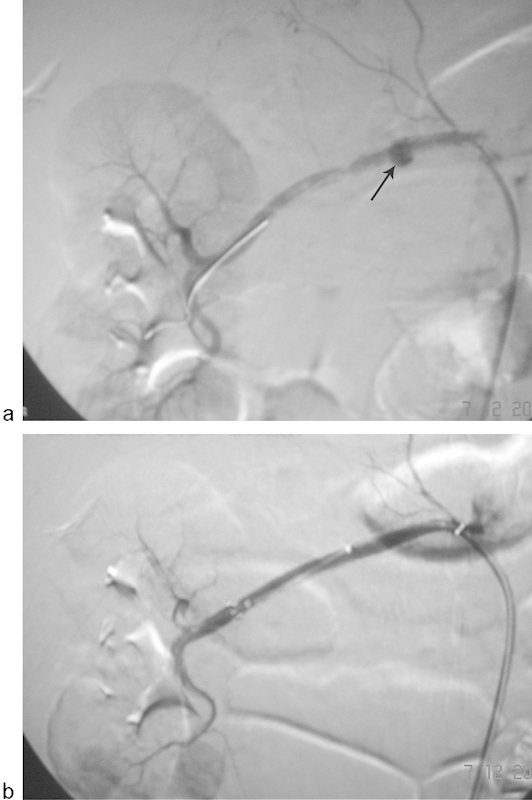
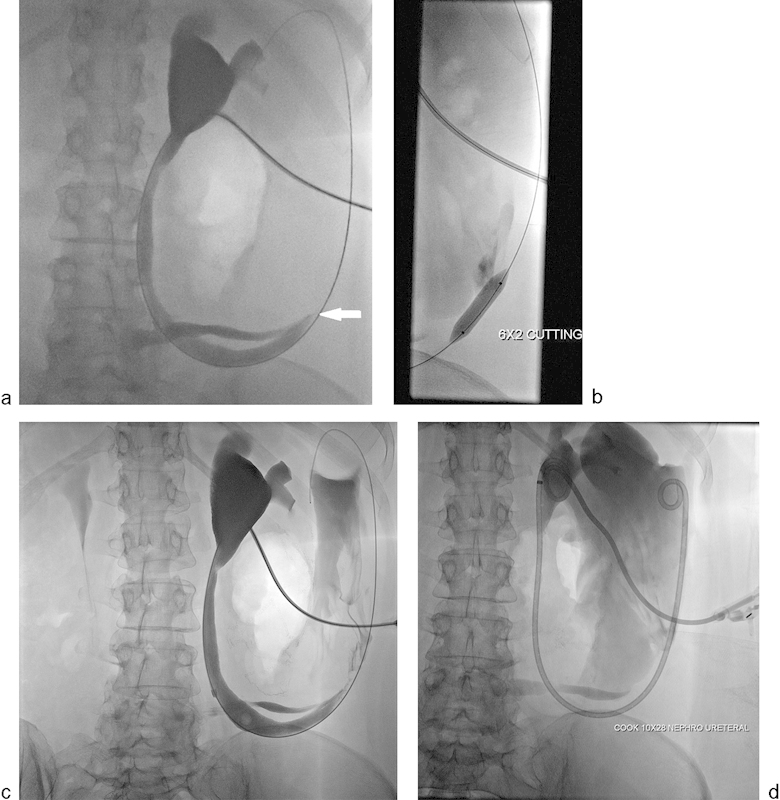
Iatrogenic injury to the urinary tract, including the kidneys, ureters, bladder, and urethra, is a potential complication of surgical procedures performed in or around the retroperitoneal abdominal space or pelvis. While both diagnostic and interventional radiologists often play a central and decisive role in the identification and initial management of a variety of iatrogenic injuries, discussions of these injuries are often directed toward specialists such as urologists, obstetricians, gynecologists, and general surgeons whose procedures are most often implicated in iatrogenic urinary tract injuries. Interventional radiologic procedures can also be a source of an iatrogenic urinary tract injury. This review describes the clinical presentation, risk factors, imaging findings, and management of iatrogenic renal vascular and urinary tract injuries, as well as the radiologist's role in the diagnosis, treatment, and cause of these injuries.
Keywords: bladder; iatrogenic injury; interventional radiology; renal vascular; ureter.
Conflict of interest statement
Figures






References
-
- Selzman A A, Spirnak J P. Iatrogenic ureteral injuries: a 20-year experience in treating 165 injuries. J Urol. 1996;155(3):878–881. - PubMed
-
- Summerton D J Kitrey N D Lumen N Serafetinidis E Djakovic N; European Association of Urology. EAU guidelines on iatrogenic trauma Eur Urol 2012624628–639. - PubMed
-
- Brandes S, Coburn M, Armenakas N, McAninch J. Diagnosis and management of ureteric injury: an evidence-based analysis. BJU Int. 2004;94(3):277–289. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
