

Trends in Transmission of Drug Resistance and Prevalence of Non-B Subtypes in Patients with Acute or Recent HIV-1 Infection in Barcelona in the Last 16 Years (1997-2012)
- PMID: 26039689
- PMCID: PMC4454638
- DOI: 10.1371/journal.pone.0125837
Trends in Transmission of Drug Resistance and Prevalence of Non-B Subtypes in Patients with Acute or Recent HIV-1 Infection in Barcelona in the Last 16 Years (1997-2012)
Abstract
Objectives: To evaluate the prevalence of transmitted drug resistance (TDR) and non-B subtypes in patients with acute/recent HIV-1 infection in Barcelona during the period 1997-2012.
Methods: Patients from the "Hospital Clínic Primary HIV-1 Infection Cohort" with a genotyping test performed within 180 days of infection were included. The 2009 WHO List of Mutations for Surveillance of Transmitted HIV-1 Drug Resistance was used for estimating the prevalence of TDR and phylogenetic analysis for subtype determination.
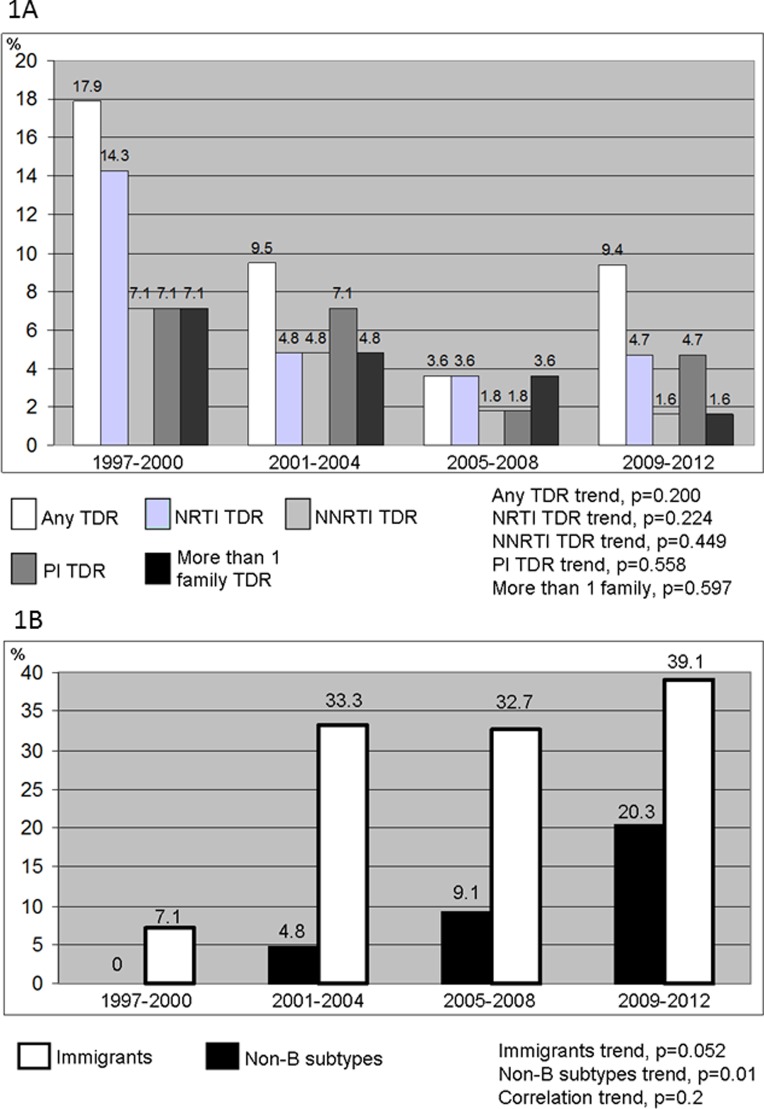
Results: 189 patients with acute/recent HIV-1 infection were analyzed in 4 time periods (1997-2000, n=28; 2001-4, n=42; 2005-8, n=55 and 2009-12, n=64). The proportion of patients with acute/recent HIV-1 infection with respect to the total of newly HIV-diagnosed patients in our center increased over the time and was 2.18%, 3.82%, 4.15% and 4.55% for the 4 periods, respectively (p=0.005). The global prevalence of TDR was 9%, or 17.9%, 9.5%, 3.6% and 9.4% by study period (p=0.2). The increase in the last period was driven by protease-inhibitor and nucleoside-reverse-transcriptase-inhibitor resistance mutations while non-nucleoside-reverse-transcriptase inhibitor TDR and TDR of more than one family decreased. The overall prevalence of non-B subtypes was 11.1%, or 0%, 4.8%, 9.1% and 20.3 by study period (p=0.01). B/F recombinants, B/G recombinants and subtype F emerged in the last period. We also noticed an increase in the number of immigrant patients (p=0.052). The proportion of men-who-have-sex-with-men (MSM) among patients with acute/recent HIV-1 infection increased over the time (p=0.04).
Conclusions: The overall prevalence of TDR in patients with acute/recent HIV-1 infection in Barcelona was 9%, and it has stayed relatively stable in recent years. Non-B subtypes and immigrants proportions progressively increased.
Conflict of interest statement
Figures

References
-
- Harrigan PR, Hogg RS, Dong WW, Yip B, Wynhoven B, Woodward J, et al. Predictors of HIV drug-resistance mutations in a large antiretroviral-naive cohort initiating triple antiretroviral therapy. J Infect Dis 2005; 191:339–347. - PubMed
-
- Booth CL, Geretti AM. Prevalence and determinants of transmitted antiretroviral drug resistance in HIV-1 infection. J Antimicrob Chemother 2007; 59:1047–1056. - PubMed
-
- Girardi E. Epidemiological aspects of transmitted HIV drug resistance. Scand J Infect Dis Suppl 2003; 106:17–20. - PubMed
-
- Hecht FM, Wang L, Collier A, Little S, Markowitz M, Margolick J, et al. A multicenter observational study of the potential benefits of initiating combination antiretroviral therapy during acute HIV infection. J Infect Dis 2006; 194:725–733. - PubMed
-
- Smith D, Moini N, Pesano R, Cachay E, Aiem H, Lie Y, et al. Clinical utility of HIV standard genotyping among antiretroviral-naive individuals with unknown duration of infection. Clin Infect Dis 2007; 44:456–458. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
