

Reducing the global burden of type 2 diabetes by improving the quality of staple foods: The Global Nutrition and Epidemiologic Transition Initiative
- PMID: 26040275
- PMCID: PMC4489001
- DOI: 10.1186/s12992-015-0109-9
Reducing the global burden of type 2 diabetes by improving the quality of staple foods: The Global Nutrition and Epidemiologic Transition Initiative
Abstract
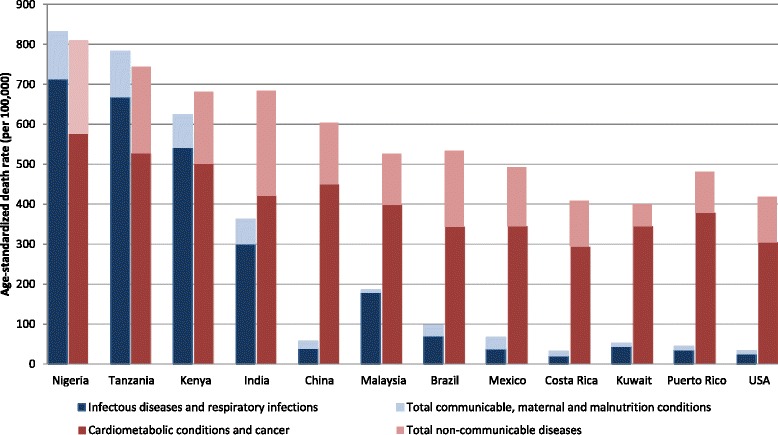
Background: The prevalence of type 2 diabetes has been reaching epidemic proportions across the globe, affecting low/middle-income and developed countries. Two main contributors to this burden are the reduction in mortality from infectious conditions and concomitant negative changes in lifestyles, including diet. We aimed to depict the current state of type 2 diabetes worldwide in light of the undergoing epidemiologic and nutrition transition, and to posit that a key factor in the nutrition transition has been the shift in the type and processing of staple foods, from less processed traditional foods to highly refined and processed carbohydrate sources.
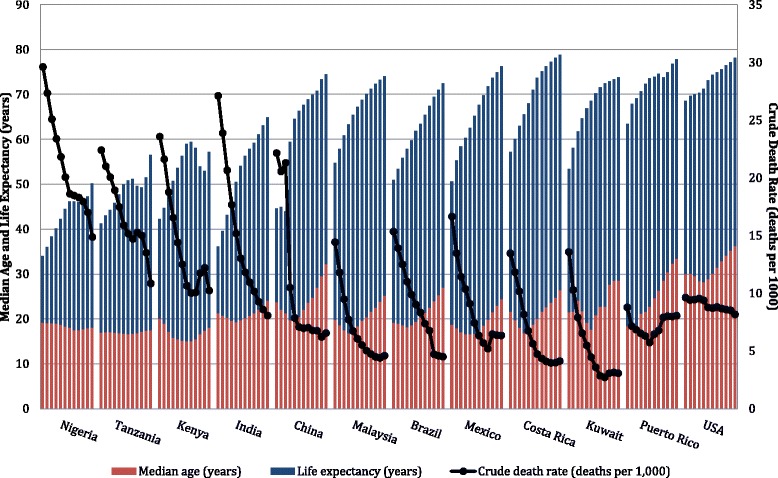
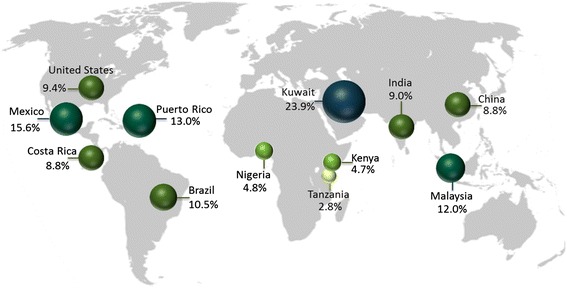
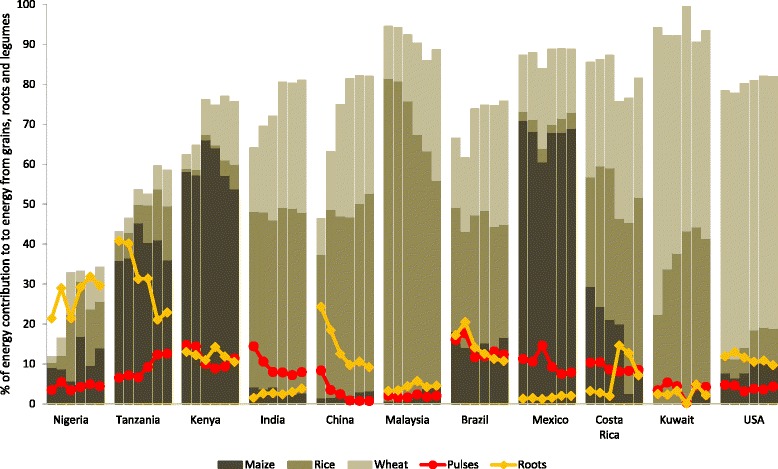
Discussion: We showed data from 11 countries participating in the Global Nutrition and Epidemiologic Transition Initiative, a collaborative effort across countries at various stages of the nutrition-epidemiologic transition whose mission is to reduce diabetes by improving the quality of staple foods through culturally-appropriate interventions. We depicted the epidemiologic transition using demographic and mortality data from the World Health Organization, and the nutrition transition using data from the Food and Agriculture Organization food balance sheets. Main staple foods (maize, rice, wheat, pulses, and roots) differed by country, with most countries undergoing a shift in principal contributors to energy consumption from grains in the past 50 years. Notably, rice and wheat products accounted for over half of the contribution to energy consumption from staple grains, while the trends for contribution from roots and pulses generally decreased in most countries. Global Nutrition and Epidemiologic Transition Initiative countries with pilot data have documented key barriers and motivators to increase intake of high-quality staple foods. Global research efforts to identify and promote intake of culturally-acceptable high-quality staple foods could be crucial in preventing diabetes. These efforts may be valuable in shaping future research, community interventions, and public health and nutritional policies.
Figures
References
-
- International Diabetes Federation. IDF Diabetes Atlas. 2013. http://www.idf.org/sites/default/files/EN_6E_Atlas_Full_0.pdf. Accessed: 18 Sept 2014.
-
- World Health Organization. Diabetes factsheet. 2013. http://www.who.int/mediacentre/factsheets/fs312/en/. Accessed: 18 Sept 2014.
-
- Danaei G, Finucane MM, Lu Y, Singh GM, Cowan MJ, Paciorek CJ, et al. National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2.7 million participants. Lancet. 2011;378(9785):31–40. - PubMed
-
- Hossain P, Kawar B, El Nahas M. Obesity and diabetes in the developing world–a growing challenge. N Engl J Med. 2007;356(3):213–5. - PubMed
-
- Omran AR. The epidemiologic transition. A theory of the epidemiology of population change. Milbank Mem Fund Q. 1971;49(4):509––38. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
