

The Minimum Clinically Important Difference of the Patient-rated Wrist Evaluation Score for Patients With Distal Radius Fractures
- PMID: 26040969
- PMCID: PMC4562929
- DOI: 10.1007/s11999-015-4376-9
The Minimum Clinically Important Difference of the Patient-rated Wrist Evaluation Score for Patients With Distal Radius Fractures
Erratum in
-
Erratum to: The Minimum Clinically Important Difference of the Patient-rated Wrist Evaluation Score for Patients With Distal Radius Fractures.Clin Orthop Relat Res. 2015 Sep;473(9):3063. doi: 10.1007/s11999-015-4444-1. Clin Orthop Relat Res. 2015. PMID: 26155768 Free PMC article. No abstract available.
Abstract
Background: The Patient-rated Wrist Evaluation (PRWE) is a commonly used instrument in upper extremity surgery and in research. However, to recognize a treatment effect expressed as a change in PRWE, it is important to be aware of the minimum clinically important difference (MCID) and the minimum detectable change (MDC). The MCID of an outcome tool like the PRWE is defined as the smallest change in a score that is likely to be appreciated by a patient as an important change, while the MDC is defined as the smallest amount of change that can be detected by an outcome measure. A numerical change in score that is less than the MCID, even when statistically significant, does not represent a true clinically relevant change. To our knowledge, the MCID and MDC of the PRWE have not been determined in patients with distal radius fractures.
Questions/purposes: We asked: (1) What is the MCID of the PRWE score for patients with distal radius fractures? (2) What is the MDC of the PRWE?
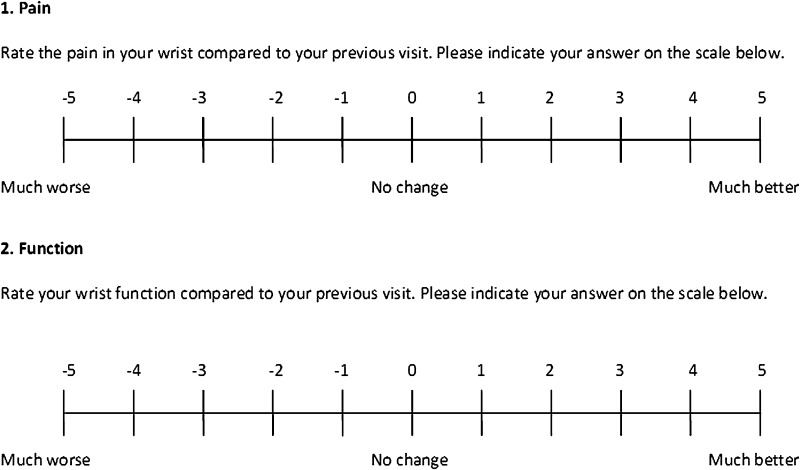
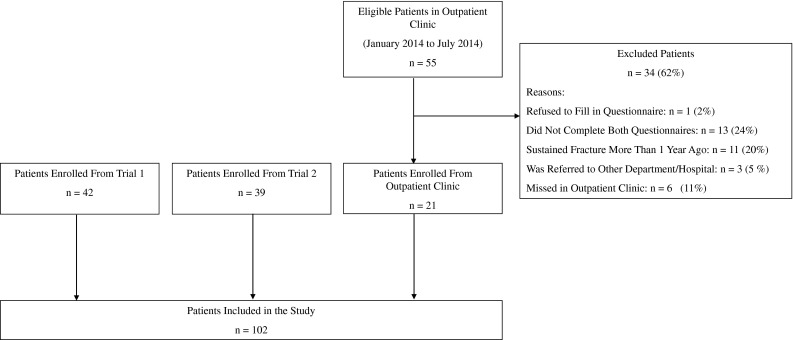
Methods: Our prospective cohort study included 102 patients with a distal radius fracture and a median age of 59 years (interquartile range [IQR], 48-66 years). All patients completed the PRWE questionnaire during each of two separate visits. At the second visit, patients were asked to indicate the degree of clinical change they appreciated since the previous visit. Accordingly, patients were categorized in two groups: (1) minimally improved or (2) no change. The groups were used to anchor the changes observed in the PRWE score to patients' perspectives of what was clinically important. We determined the MCID using an anchor-based receiver operator characteristic method. In this context, the change in the PRWE score was considered a diagnostic test, and the anchor (minimally improved or no change as noted by the patients from visit to visit) was the gold standard. The optimal receiver operator characteristic cutoff point calculated with the Youden index reflected the value of the MCID.
Results: In our study, the MCID of the PRWE was 11.5 points. The area under the curve was 0.54 (95% CI, 0.37-0.70) for the pain subscale and 0.71 (95% CI, 0.57-0.85) for the function subscale. We determined the MDC to be 11.0 points.
Conclusions: We determined the MCID of the PRWE score for patients with distal radius fractures using the anchor-based approach and verified that the MDC of the PRWE was sufficiently small to detect our MCID.
Clinical relevance: We recommend using an improvement on the PRWE of more than 11.5 points as the smallest clinically relevant difference when evaluating the effects of treatments and when performing sample-size calculations on studies of distal radius fractures.
Figures
Comment in
-
CORR Insights: The Minimum Clinically Important Difference of the Patient-rated Wrist Evaluation Score for Patients With Distal Radius Fractures.Clin Orthop Relat Res. 2015 Oct;473(10):3242-4. doi: 10.1007/s11999-015-4452-1. Epub 2015 Jul 30. Clin Orthop Relat Res. 2015. PMID: 26224290 Free PMC article. No abstract available.
References
-
- Beaton DE, Bombardier C, Katz JN, Wright JG, Wells G, Boers M, Strand V, Shea B. Looking for important change/differences in studies of responsiveness. OMERACT MCID Working Group. Outcome measures in rheumatology: minimal clinically important difference. J Rheumatol. 2001;28:400–405. - PubMed
-
- Beerekamp MS, Ubbink DT, Maas M, Luitse JS, Kloen P, Blokhuis TJ, Segers MJ, Marmor M, Schep NW, Dijkgraaf MG, Goslings JC. Project group of the EF3X-trial. Fracture surgery of the extremities with the intra-operative use of 3D-RX: q randomized multicenter trial (EF3X-trial) BMC Musculoskelet Disord. 2011;12:151. doi: 10.1186/1471-2474-12-151. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
