

Continuous central venous oxygen saturation assisted intraoperative hemodynamic management during major abdominal surgery: a randomized, controlled trial
- PMID: 26041437
- PMCID: PMC4453106
- DOI: 10.1186/s12871-015-0064-2
Continuous central venous oxygen saturation assisted intraoperative hemodynamic management during major abdominal surgery: a randomized, controlled trial
Abstract
Background: Major abdominal surgery is associated with significant risk of morbidity and mortality in the perioperative period. Optimising intraoperative fluid administration may result in improved outcomes. Our aim was to compare the effects of central venous pressure (CVP), and central venous oxygen saturation (ScvO2)-assisted fluid therapy on postoperative complications in patients undergoing high risk surgery.
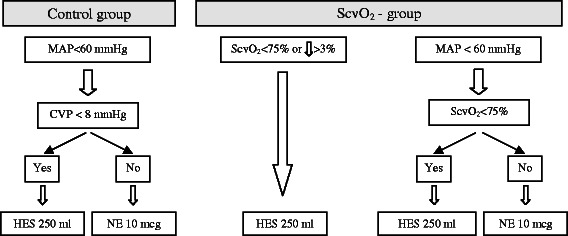
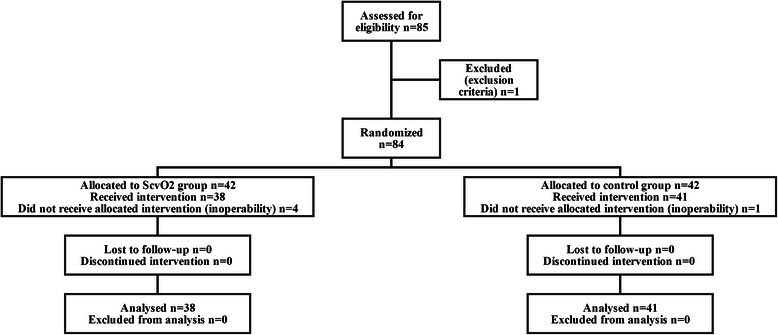
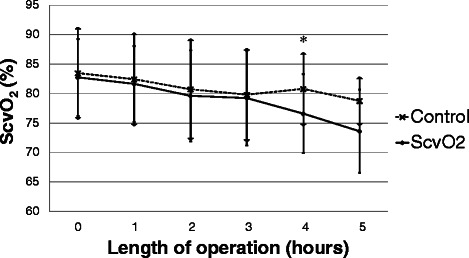
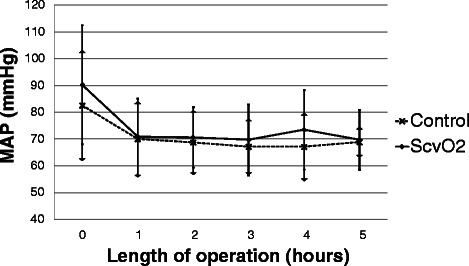
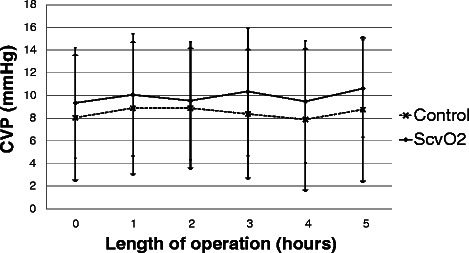
Methods: Patients undergoing elective major abdominal surgery were randomised into control and ScvO2 groups. The target level of mean arterial pressure (MAP) was ≥ 60 mmHg in both groups. In cases of MAP < 60 mmHg patients received either a fluid or vasopressor bolus according to the CVP < 8 mmHg in the control group. In the ScvO2 group, in addition to the MAP, an ScvO2 of <75% or a >3% decrease indicated need for intervention, regardless of the actual MAP. Data are presented as mean ± standard deviation or median (interquartile range).
Results: We observed a lower number of patients with complications in the ScvO2 group compared to the control group, however it did not reach statistical significance (ScvO2 group: 10 vs.
Control group: 19; p = 0.07). Patients in the ScvO2 group (n = 38) received more colloids compared to the control group (n = 41) [279(161) vs. 107(250) ml/h; p < 0.001]. Both groups received similar amounts of crystalloid (1126 ± 471 vs. 1049 ± 431 ml/h; p = 0.46) and norepinephrine [37(107) vs. 18(73) mcg/h; p = 0.84]. Despite similar blood loss in both groups, the ScvO2 group received more blood transfusions (63% vs. 37%; p = 0.018). More patients in the control group had a postoperative PaO2/FiO2 < 200 mmHg (23 vs. 10, p < 0.01). Twenty eight day survival was significantly higher in the ScvO2 group (37/38 vs. 33/41 p = 0.018).
Conclusion: ScvO2-assisted intraoperative haemodynamic support provided some benefits, including significantly better postoperative oxygenation and 28 day survival rate, compared to CVP-assisted therapy without a significant effect on postoperative complications during major abdominal surgery.
Trial registration: ClinicalTrials.gov NCT02337010.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
