

Relief and Recurrence of Congestion During and After Hospitalization for Acute Heart Failure: Insights From Diuretic Optimization Strategy Evaluation in Acute Decompensated Heart Failure (DOSE-AHF) and Cardiorenal Rescue Study in Acute Decompensated Heart Failure (CARESS-HF)
- PMID: 26041600
- PMCID: PMC4512849
- DOI: 10.1161/CIRCHEARTFAILURE.114.001957
Relief and Recurrence of Congestion During and After Hospitalization for Acute Heart Failure: Insights From Diuretic Optimization Strategy Evaluation in Acute Decompensated Heart Failure (DOSE-AHF) and Cardiorenal Rescue Study in Acute Decompensated Heart Failure (CARESS-HF)
Abstract
Background: Congestion is the most frequent cause for hospitalization in acute decompensated heart failure. Although decongestion is a major goal of acute therapy, it is unclear how the clinical components of congestion (eg, peripheral edema, orthopnea) contribute to outcomes after discharge or how well decongestion is maintained.
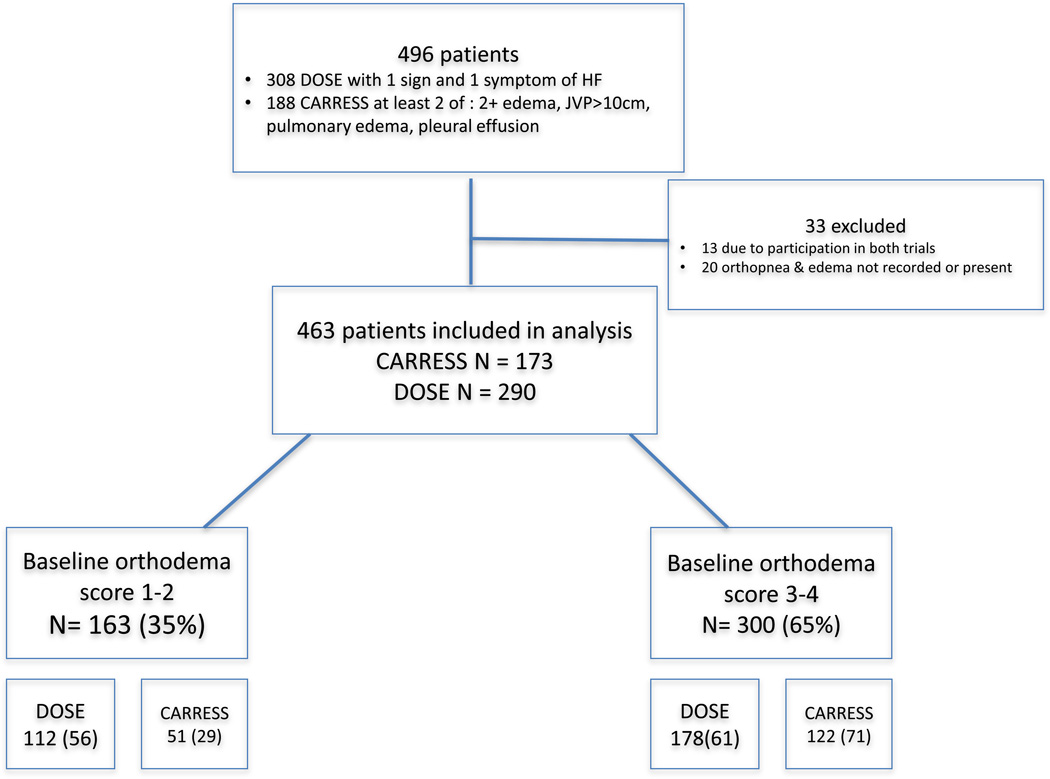
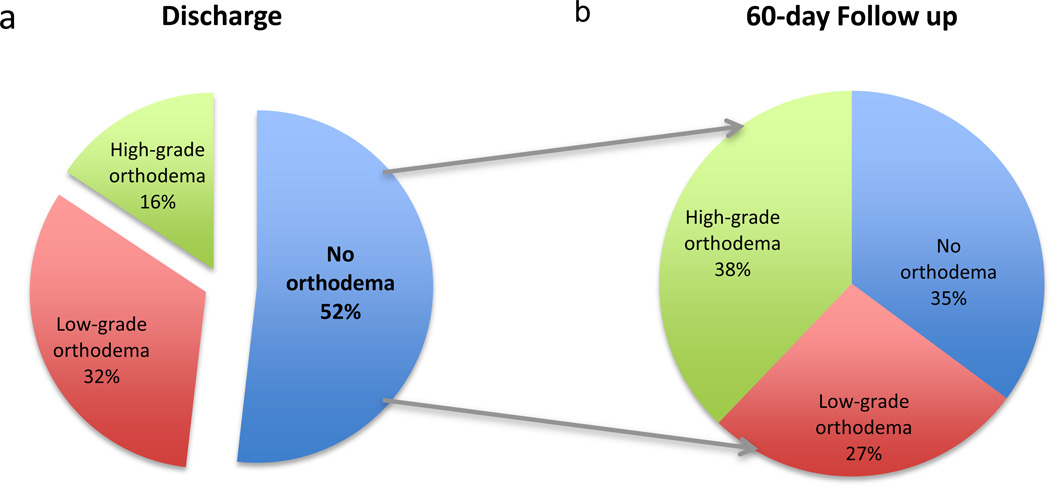
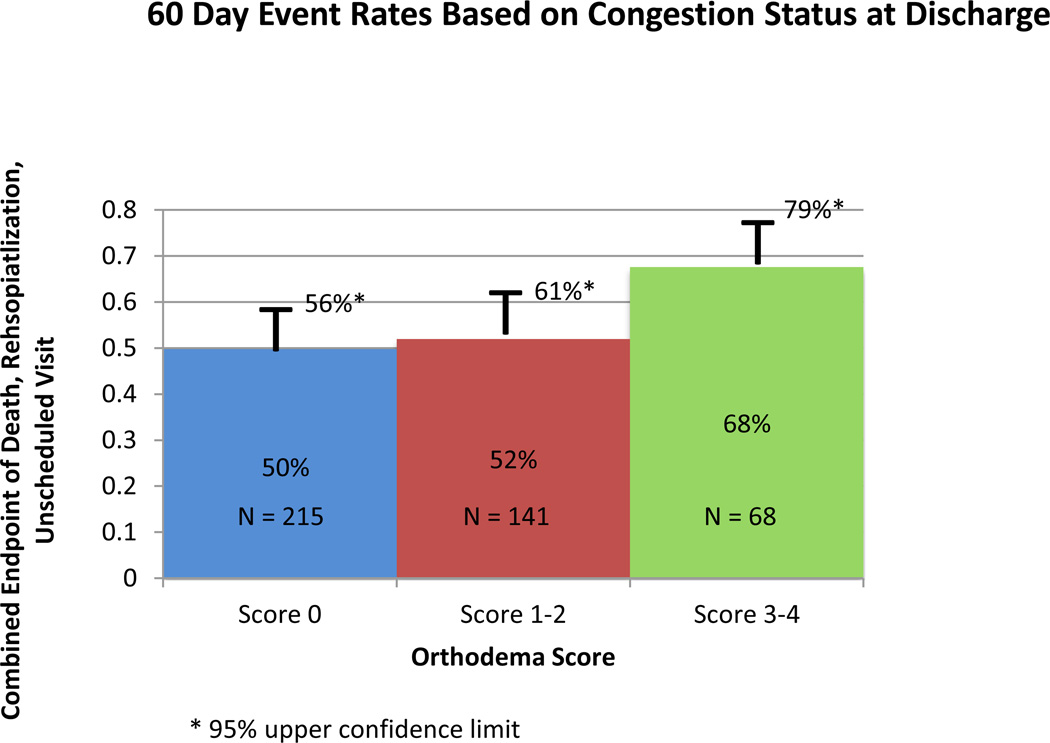
Methods and results: A post hoc analysis was performed of 496 patients enrolled in the Diuretic Optimization Strategy Evaluation in Acute Decompensated Heart Failure (DOSE-AHF) and Cardiorenal Rescue Study in Acute Decompensated Heart Failure (CARRESS-HF) trials during hospitalization with acute decompensated heart failure and clinical congestion. A simple orthodema congestion score was generated based on symptoms of orthopnea (≥2 pillows=2 points, <2 pillows=0 points) and peripheral edema (trace=0 points, moderate=1 point, severe=2 points) at baseline, discharge, and 60-day follow-up. Orthodema scores were classified as absent (score of 0), low-grade (score of 1-2), and high-grade (score of 3-4), and the association with death, rehospitalization, or unscheduled medical visits through 60 days was assessed. At baseline, 65% of patients had high-grade orthodema and 35% had low-grade orthodema. At discharge, 52% patients were free from orthodema at discharge (score=0) and these patients had lower 60-day rates of death, rehospitalization, or unscheduled visits (50%) compared with those with low-grade or high-grade orthodema (52% and 68%, respectively; P=0.038). Of the patients without orthodema at discharge, 27% relapsed to low-grade orthodema and 38% to high-grade orthodema at 60-day follow-up.
Conclusions: Increased severity of congestion by a simple orthodema assessment is associated with increased morbidity and mortality. Despite intent to relieve congestion, current therapy often fails to relieve orthodema during hospitalization or to prevent recurrence after discharge.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifiers: NCT00608491, NCT00577135.
Keywords: dyspnea; edema; follow-up studies; heart failure; hospitalization.
© 2015 American Heart Association, Inc.
Conflict of interest statement
The other authors report no relevant conflicts of interest.
Figures
References
-
- Braunwald E. Heart Failure. JACC Heart failure. 2013;1:1–20. - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Jr, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, Johnson MR, Kasper EK, Levy WC, Masoudi FA, McBride PE, McMurray JJ, Mitchell JE, Peterson PN, Riegel B, Sam F, Stevenson LW, Tang WH, Tsai EJ, Wilkoff BL. American College of Cardiology F and American Heart Association Task Force on Practice G. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology. 2013;62:e147–e239. - PubMed
-
- Felker GM, Lee KL, Bull DA, Redfield MM, Stevenson LW, Goldsmith SR, LeWinter MM, Deswal A, Rouleau JL, Ofili EO, Anstrom KJ, Hernandez AF, McNulty SE, Velazquez EJ, Kfoury AG, Chen HH, Givertz MM, Semigran MJ, Bart BA, Mascette AM, Braunwald E, O’Connor CM. Network NHFCR Diuretic strategies in patients with acute decompensated heart failure. The New England journal of medicine. 2011;364:797–805. - PMC - PubMed
-
- Bart BA, Goldsmith SR, Lee KL, Givertz MM, O’Connor CM, Bull DA, Redfield MM, Deswal A, Rouleau JL, LeWinter MM, Ofili EO, Stevenson LW, Semigran MJ, Felker GM, Chen HH, Hernandez AF, Anstrom KJ, McNulty SE, Velazquez EJ, Ibarra JC, Mascette AM, Braunwald E, Heart Failure Clinical Research N. Ultrafiltration in decompensated heart failure with cardiorenal syndrome. The New England journal of medicine. 2012;367:2296–2304. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
