

Plasma insulin profiles after subcutaneous injection: how close can we get to physiology in people with diabetes?
- PMID: 26041603
- PMCID: PMC4744667
- DOI: 10.1111/dom.12501
Plasma insulin profiles after subcutaneous injection: how close can we get to physiology in people with diabetes?
Abstract
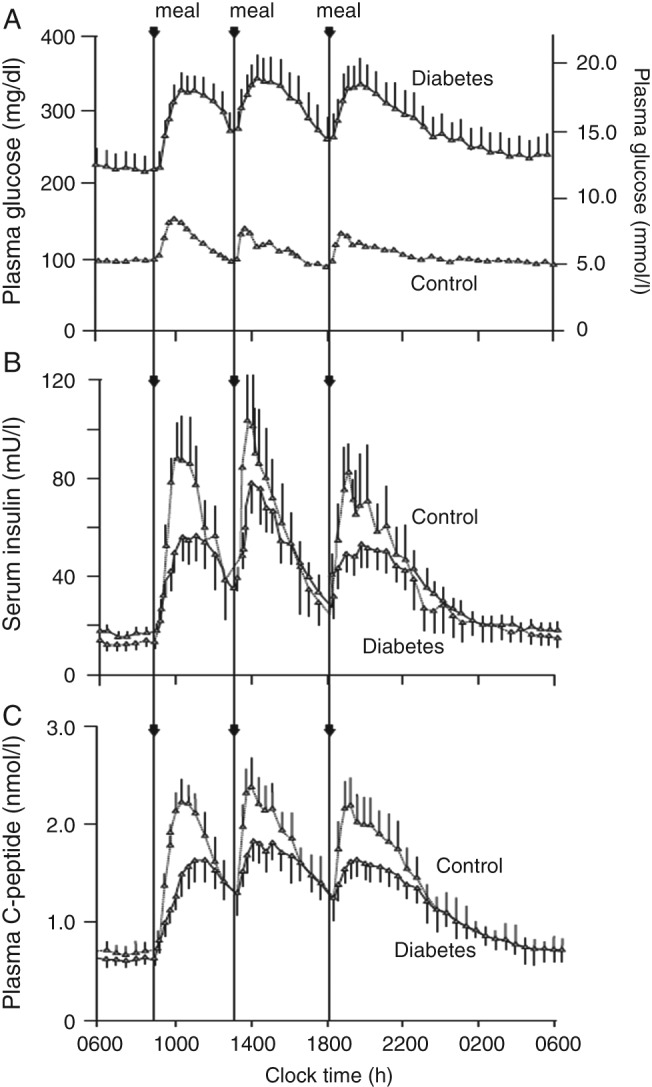
Many people with diabetes rely on insulin therapy to achieve optimal blood glucose control. A fundamental aim of such therapy is to mimic the pattern of 'normal' physiological insulin secretion, thereby controlling basal and meal-time plasma glucose and fatty acid turnover. In people without diabetes, insulin release is modulated on a time base of 3-10 min, something that is impossible to replicate without intravascular glucose sensing and insulin delivery. Overnight physiological insulin delivery by islet β cells is unchanging, in contrast to requirements once any degree of hyperglycaemia occurs, when diurnal influences are evident. Subcutaneous pumped insulin or injected insulin analogues can approach the physiological profile, but there remains the challenge of responding to day-to-day changes in insulin sensitivity. Physiologically, meal-time insulin release begins rapidly in response to reflex activity and incretins, continuing with the rise in glucose and amino acid concentrations. This rapid response reflects the need to fill the insulin space with maximum concentration as early as 30 min after starting the meal. Current meal-time insulins, by contrast, are associated with a delay after injection before absorption begins, and a delay to peak because of tissue diffusion. While decay from peak for monomeric analogues is not dissimilar to average physiological needs, changes in meal type and, again, in day-to-day insulin sensitivity, are difficult to match. Recent and current developments in insulin depot technology are moving towards establishing flatter basal and closer-to-average physiological meal-time plasma insulin profiles. The present article discusses the ideal physiological insulin profile, how this can be met by available and future insulin therapies and devices, and the challenges faced by healthcare professionals and people with diabetes in trying to achieve an optimum plasma insulin profile.
Keywords: analogue; basal; diabetes; insulin therapy; meal; physiology.
© 2015 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Figures

References
-
- The Diabetes Control and Complications Trial Research Group . The effect of intensive treatment of diabetes on the development and progression of long‐term complications in insulin‐dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Engl J Med 1993; 329: 977–986. - PubMed
-
- UK Prospective Diabetes Study (UKPDS) Group . Intensive blood‐glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998; 352: 837–853. - PubMed
-
- Homko C, Deluzio A, Jimenez C, Kolaczynski JW, Boden G. Comparison of insulin aspart and lispro: pharmacokinetic and metabolic effects. Diabetes Care 2003; 26: 2027–2031. - PubMed
-
- Meneghini LF. Insulin therapy for type 2 diabetes. Endocrine 2013; 43: 529–534. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
