

Eradication of B-ALL using chimeric antigen receptor-expressing T cells targeting the TSLPR oncoprotein
- PMID: 26041741
- PMCID: PMC4520878
- DOI: 10.1182/blood-2014-11-612903
Eradication of B-ALL using chimeric antigen receptor-expressing T cells targeting the TSLPR oncoprotein
Erratum in
-
Erratum: Qin H, Cho M, Haso W, et al. Eradication of B-ALL using chimeric antigen receptor-expressing T cells targeting the TSLPR oncoprotein. Blood. 2015;126(5):629-639.Blood. 2016 Sep 8;128(10):1441. doi: 10.1182/blood-2016-07-730697. Blood. 2016. PMID: 31265501 Free PMC article.
Abstract
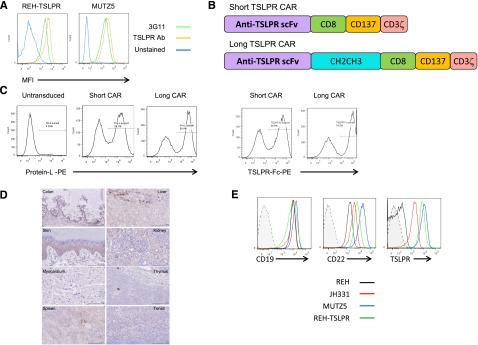
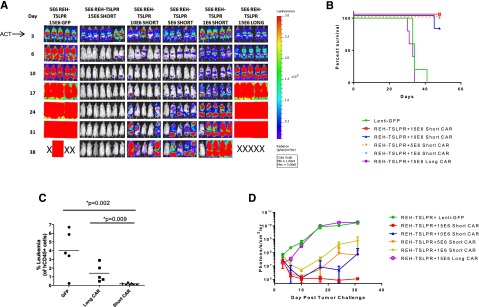
Adoptive transfer of T cells genetically modified to express chimeric antigen receptors (CARs) targeting the CD19 B cell-associated protein have demonstrated potent activity against relapsed/refractory B-lineage acute lymphoblastic leukemia (B-ALL). Not all patients respond, and CD19-negative relapses have been observed. Overexpression of the thymic stromal lymphopoietin receptor (TSLPR; encoded by CRLF2) occurs in a subset of adults and children with B-ALL and confers a high risk of relapse. Recent data suggest the TSLPR signaling axis is functionally important, suggesting that TSLPR would be an ideal immunotherapeutic target. We constructed short and long CARs targeting TSLPR and tested efficacy against CRLF2-overexpressing B-ALL. Both CARs demonstrated activity in vitro, but only short TSLPR CAR T cells mediated leukemia regression. In vivo activity of the short CAR was also associated with long-term persistence of CAR-expressing T cells. Short TSLPR CAR treatment of mice engrafted with a TSLPR-expressing ALL cell line induced leukemia cytotoxicity with efficacy comparable with that of CD19 CAR T cells. Short TSLPR CAR T cells also eradicated leukemia in 4 xenograft models of human CRLF2-overexpressing ALL. Finally, TSLPR has limited surface expression on normal tissues. TSLPR-targeted CAR T cells thus represent a potent oncoprotein-targeted immunotherapy for high-risk ALL.
Figures




Comment in
-
TSLPR: a new CAR in the showroom for B-ALL.Blood. 2015 Jul 30;126(5):567-9. doi: 10.1182/blood-2015-06-650812. Blood. 2015. PMID: 26228169 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
