

Clinical and MRI phenotype of children with MOG antibodies
- PMID: 26041801
- PMCID: PMC4669239
- DOI: 10.1177/1352458515587751
Clinical and MRI phenotype of children with MOG antibodies
Abstract
Objective: To investigate the clinical and magnetic resonance imaging (MRI) features of anti-myelin oligodendrocyte glycoprotein (MOG) antibody-seropositive pediatric demyelinating syndromes.
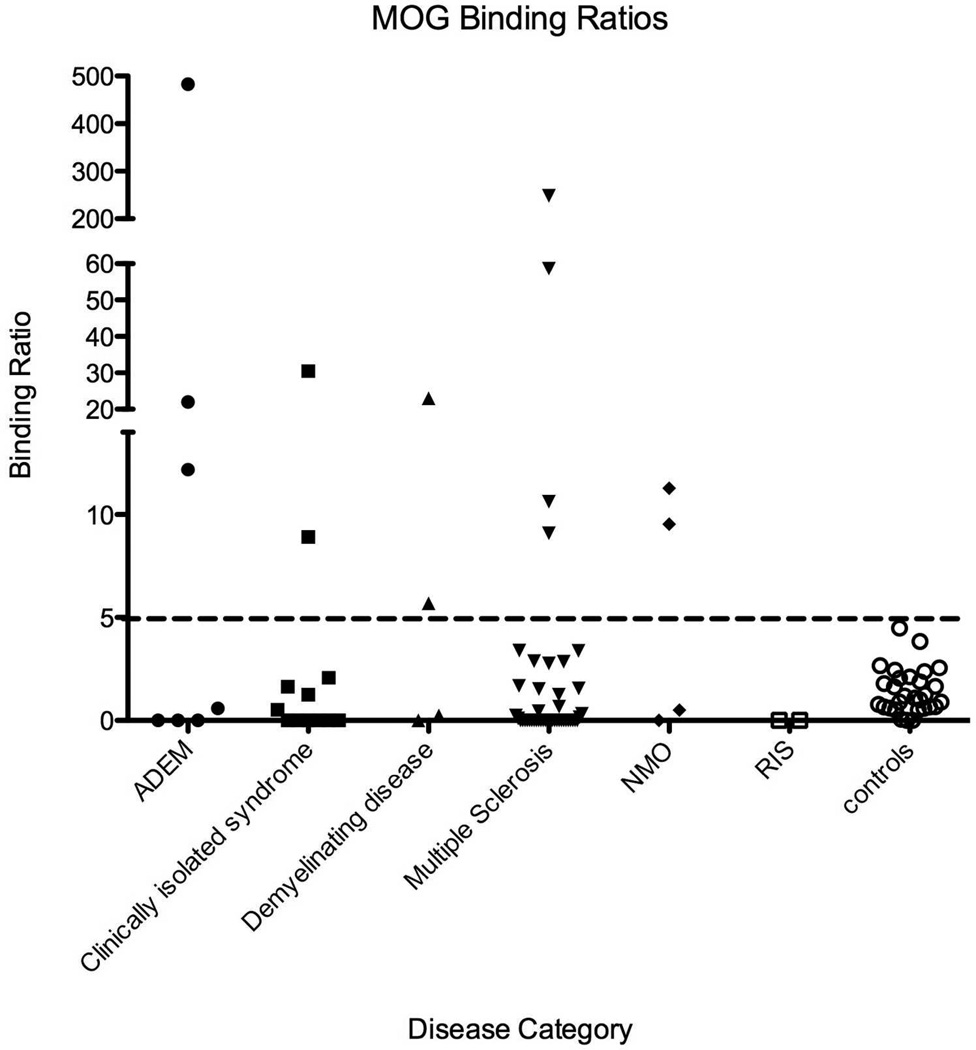
Methods: Serum samples collected from 74 children with suspected demyelinating disorders whom were being followed at Massachusetts General Hospital were incubated with control green fluorescent protein (GFP)- and MOG-GFP-transfected Jurkat cell clones. The binding ratios were calculated using flow cytometry. Using statistical analyses, we compared the demographic, clinical and radiological features in our seropositive and seronegative patients.
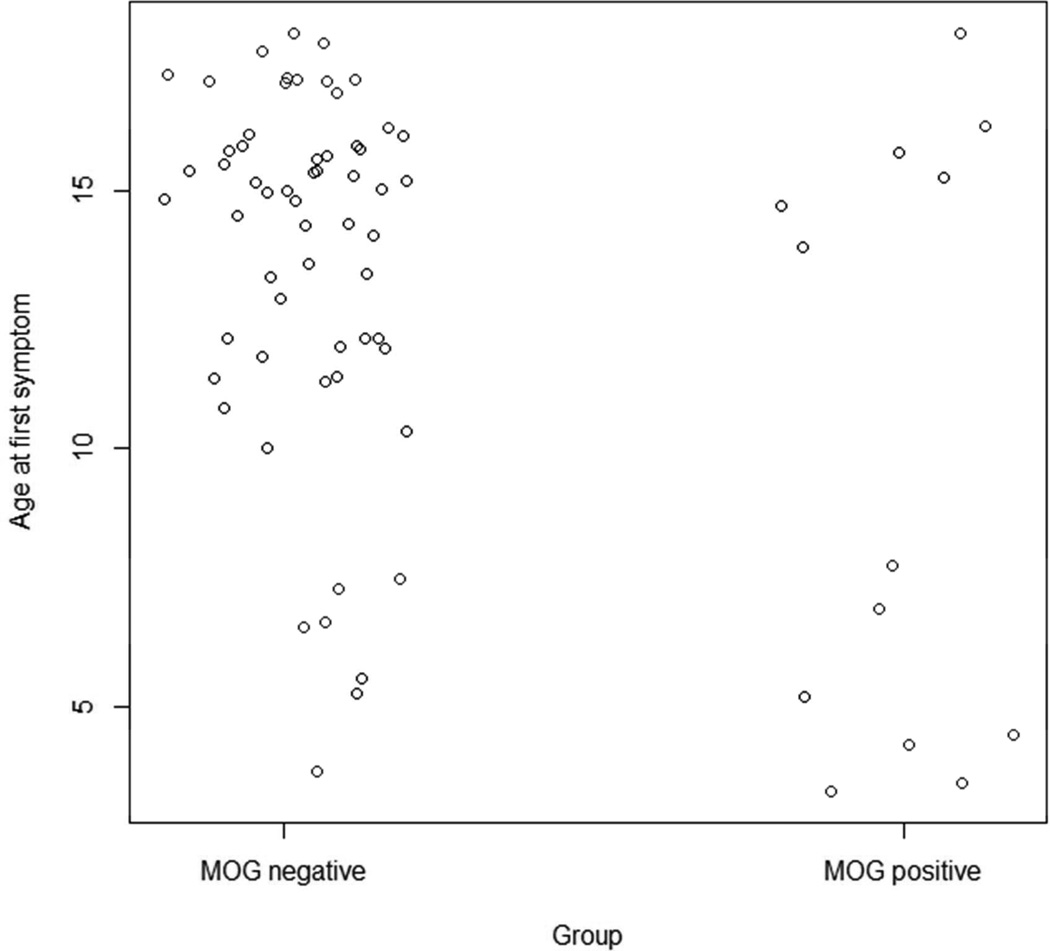
Results: We found that 13 out of 74 (17.5%) patients were seropositive for MOG. The MOG-seropositive patients were younger than the seronegative patients (p = 0.049). No single disease category predominated among the seropositive patients, nor was one group more likely to have a polyphasic course. There were two out of four neuromyelitis optica (NMO) patients who had MOG antibodies; both were seronegative for aquaporin -4 (AQP4) antibodies. One had monophasic disease and the other had frequent relapses. There was a bimodal distribution of the MOG-seropositive patients by age at onset, with a distinct younger group (4-8 years) having a high prevalence of encephalopathy and an older group (13-18 years), whom presented almost exclusively with optic neuritis. MRI analysis demonstrated the absence of corpus callosum lesions in the seropositive patients (p = 0.012). The annualized relapse rate (ARR) and the Expanded Disability Status Scale (EDSS) results at 2 years did not differ between the seropositive and seronegative patients.
Conclusion: MOG antibodies are found across a variety of pediatric demyelinating syndromes having some distinct clinical and MRI features.
Keywords: Acute disseminated encephalomyelitis; demyelinating syndromes; encephalopathy; glycoprotein; magnetic resonance imaging; multiple sclerosis; myelin; myelin oligodendrocyte glycoprotein; neuromyelitis optica; optic neuritis; pediatric multiple sclerosis; serology.
© The Author(s), 2015.
Figures
References
-
- Meinl E, Krumbholz M, Hohlfeld R. B lineage cells in the inflammatory central nervous system environment: migration, maintenance, local antibody production, and therapeutic modulation. Annals of neurology. 2006;59:880–892. - PubMed
-
- Popescu BF, Lucchinetti CF. Pathology of demyelinating diseases. Annual review of pathology. 2012;7:185–217. - PubMed
-
- Di Pauli F, Mader S, Rostasy K, et al. Temporal dynamics of anti-MOG antibodies in CNS demyelinating diseases. Clin Immunol. 2011;138:247–254. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
