

EFFICAS II: optimization of catheter contact force improves outcome of pulmonary vein isolation for paroxysmal atrial fibrillation
- PMID: 26041872
- PMCID: PMC4535556
- DOI: 10.1093/europace/euv057
EFFICAS II: optimization of catheter contact force improves outcome of pulmonary vein isolation for paroxysmal atrial fibrillation
Abstract
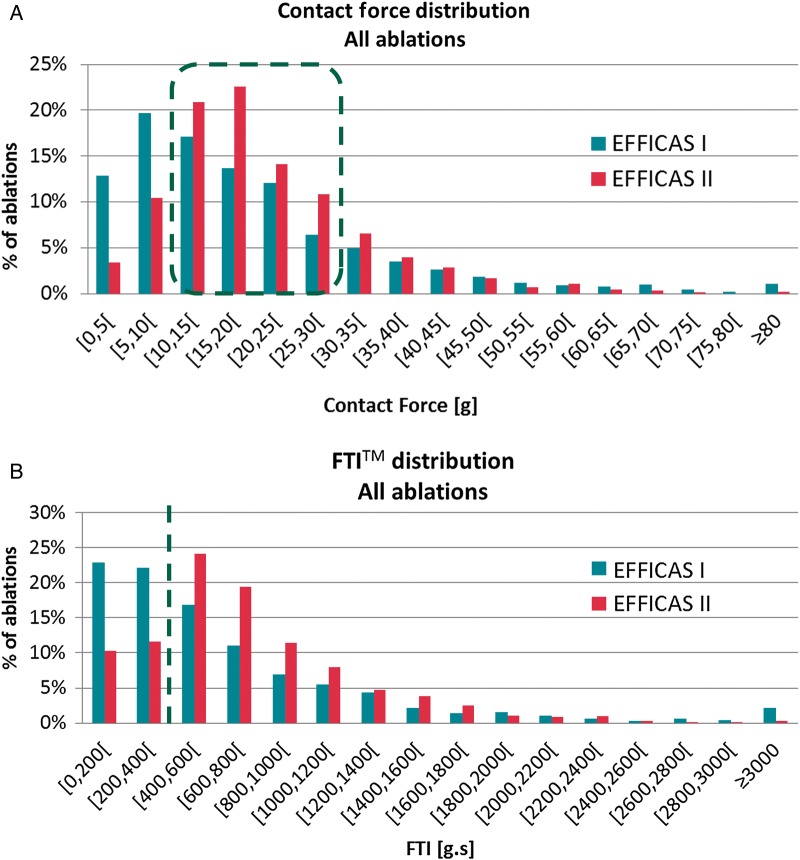
Aims: A challenge of pulmonary vein isolation (PVI) in catheter ablation for paroxysmal atrial fibrillation (PAF) is electrical reconnection of the PV. EFFICAS I showed correlation between contact force (CF) parameters and PV durable isolation but no prospective evaluation was made. EFFICAS II was a multicentre study to prospectively assess the impact of CF guidance for an effective reduction of PVI gaps.
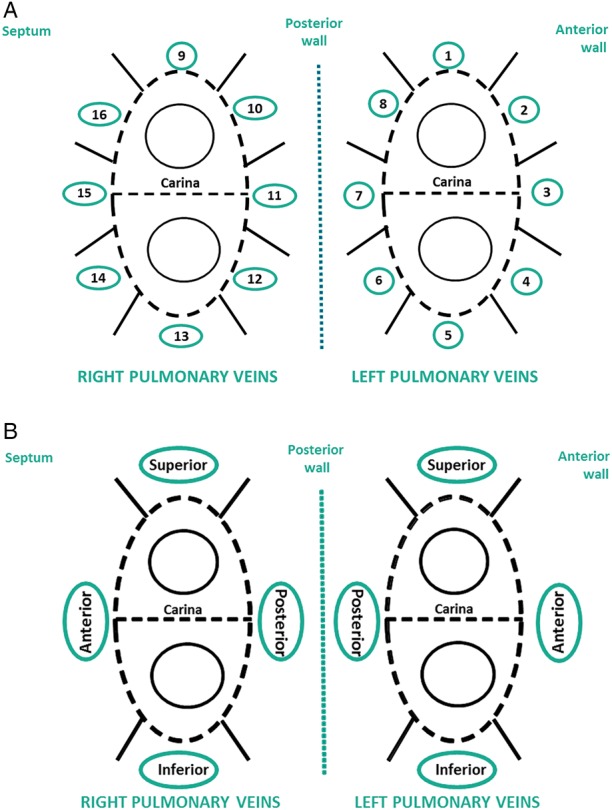
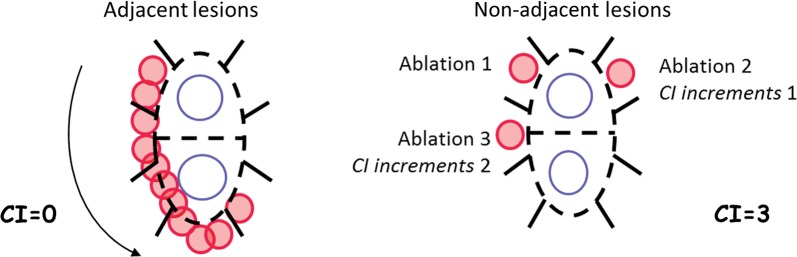
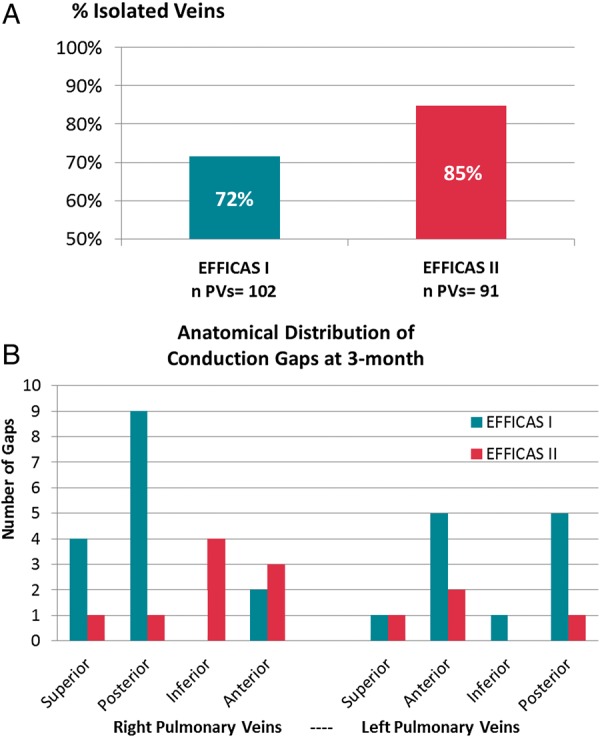
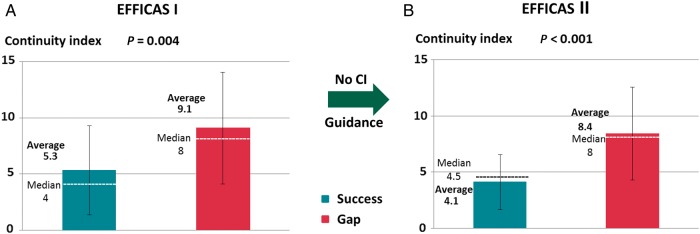
Methods and results: Pulmonary vein isolation using a radiofrequency (RF) ablation catheter with an integrated force sensor (TactiCath™) was performed in patients with PAF. Operators were provided EFFICAS I-based CF guidelines [target 20 g, range 10-30 g, minimum 400 g s force-time integral (FTI)]. Conduction gaps were assessed by remapping of PVs after 3 months, and gap rate was compared with EFFICAS I outcome. At follow up, 24 patients had 85% of PVs remaining isolated, compared with 72% in EFFICAS I (P = 0.037) in which CF guidelines were not used. The remaining 15% of gaps correlated to the number of catheter moves at creating the PVI line, quantified as Continuity Index. For PV lines with contiguous lesions and low catheter moves, durable isolation was 81% in EFFICAS I and 98% in EFFICAS II (P = 0.005). At index procedure, the number of lesions was reduced by 15% in EFFICAS II vs. EFFICAS I.
Conclusion: The use of CF with the above guidelines and contiguous deployment of RF lesions in EFFICAS II study resulted in more durable PVI in catheter ablation of PAF.
Keywords: Atrial fibrillation; Catheter ablation; Conduction gaps; Contact force; Pulmonary vein isolation.
© The Author 2015. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Towards durable pulmonary vein isolation: we are closing the gap.Europace. 2015 Aug;17(8):1164-5. doi: 10.1093/europace/euv131. Epub 2015 Jun 3. Europace. 2015. PMID: 26041871 No abstract available.
-
The contact force and continuity index parameters in pulmonary vein ablation.Europace. 2016 Apr;18(4):628. doi: 10.1093/europace/euv376. Epub 2016 Feb 8. Europace. 2016. PMID: 26857190 No abstract available.
References
-
- Santini M, Ricci RP. The worldwide social burden of atrial fibrillation: what should be done and where do we go? J Interv Card Electrophysiol 2006;17:183–8. - PubMed
-
- Ouyang F, Tilz R, Chun J, Schmidt B, Wissner E, Zerm T, et al. Long-term results of catheter ablation in paroxysmal atrial fibrillation: lessons from a 5-year follow-up. Circulation 2010;122:2368–77. - PubMed
-
- Hussein AA, Saliba WI, Martin DO, Bhargava M, Sherman M, Magnelli-Reyes C, et al. Natural history and long-term outcomes of ablated atrial fibrillation. Circ Arrhythm Electrophysiol 2011;4:271–8. - PubMed
-
- Raviele A, Natale A, Calkins H, Camm JA, Cappato R, Ann Chen S, et al. Venice Chart international consensus document on atrial fibrillation ablation: 2011 update. J Cardiovasc Electrophysiol 2012;23:890–923. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
