

Clinical neurophysiology of hepatic encephalopathy
- PMID: 26041960
- PMCID: PMC4442865
- DOI: 10.1016/j.jceh.2014.06.007
Clinical neurophysiology of hepatic encephalopathy
Abstract
Background/objectives: Hepatic encephalopathy (HE) has relevant impact on the quality of life of patients and their caregivers and causes relevant costs because of hospitalizations and work days lost. Its quantification is important to perform adequate clinical trials on this relevant complication of cirrhosis and portal-systemic shunting. Clinical neurophysiology, which detects functional alterations of the nervous system, has been applied to the study of HE for over 60 years. This review aims at summarizing and clarifying the role of neurophysiologic techniques in the study of HE.
Methods: A narrative review was performed aiming at interpreting the cited papers and the techniques on the basis of their physiological and pathophysiological meaning.
Results: The potential role of EEG, quantified EEG, evoked potentials-both exogenous, endogenous and motor-have been clarified to the reader that may be unfamiliar with neurophysiology.
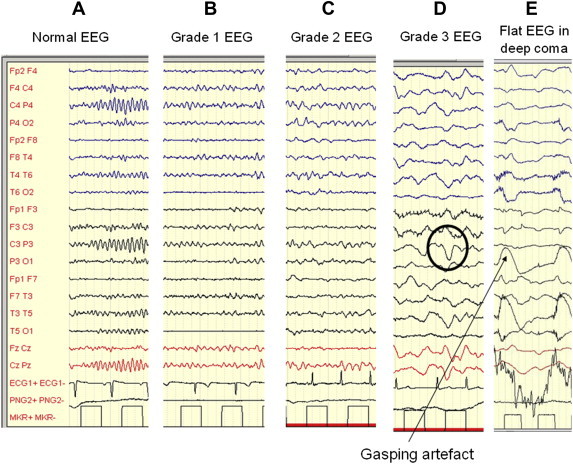
Conclusions: The EEG, reflecting the oscillatory changes of neural network is the preferable tool to detect and monitor HE, with the exception of its most severe stage, when EEG flattens. SSEP and MEP have indication to detect and monitor transmission alterations that are likely related to myelin changes and microedema.
Keywords: BAEPs, brainstem acoustic evoked potentials; EEG; EEG, electroencephalogram; EPs, evoked potentials; ERPs, event related potentials; HE, hepatic encephalopathy; MEG, magnetoencephalogram; MEPs, motor evoked potentials; SSEPs, somatosensory evoked potential; VEPs, visual evoked potentials; cirrhosis; evoked potentials; fVPS, flash visual evoked potentials; hepatic encephalopathy; neurophysiology; pVEPs, pattern reversal visual evoked potentials.
Figures
References
-
- Parsons-Smith B.G., Summerskill W.H.J., Dawson A.M., Sherlock S. The electroencephalograph in liver disease. Lancet. 1957:867–871. - PubMed
-
- Montagnese S., Jackson C., Morgan M.Y. Spatio-temporal decomposition of the electroencephalogram in patients with cirrhosis. J Hepatol. 2007;46:447–458. - PubMed
-
- Kalauzi A., Vuckovic A., Bojic T. EEG alpha phase shifts during transition from wakefulness to drowsiness. Int J Psychophysiol. 2012;86:195–205. - PubMed
-
- Sagales T., Gimeno V., de lC., Casellas F., Dolors M.M., Villar S.M. Brain mapping analysis in patients with hepatic encephalopathy. Brain Topogr. 1990;2:221–228. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
