

What factors might have led to the emergence of Ebola in West Africa?
- PMID: 26042592
- PMCID: PMC4456362
- DOI: 10.1371/journal.pntd.0003652
What factors might have led to the emergence of Ebola in West Africa?
Abstract
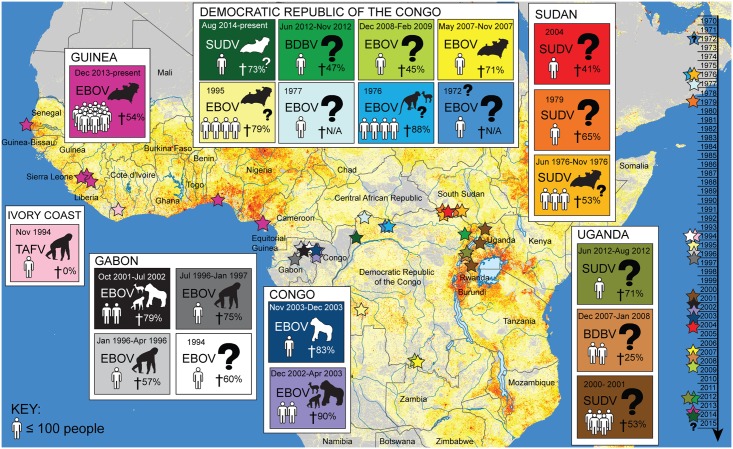
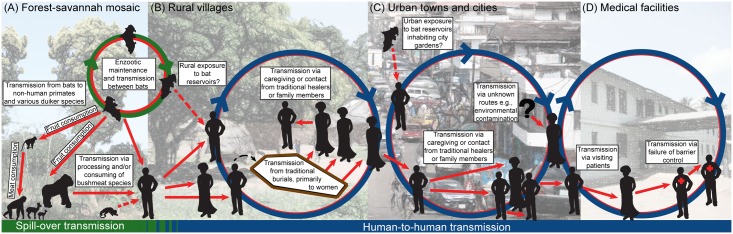
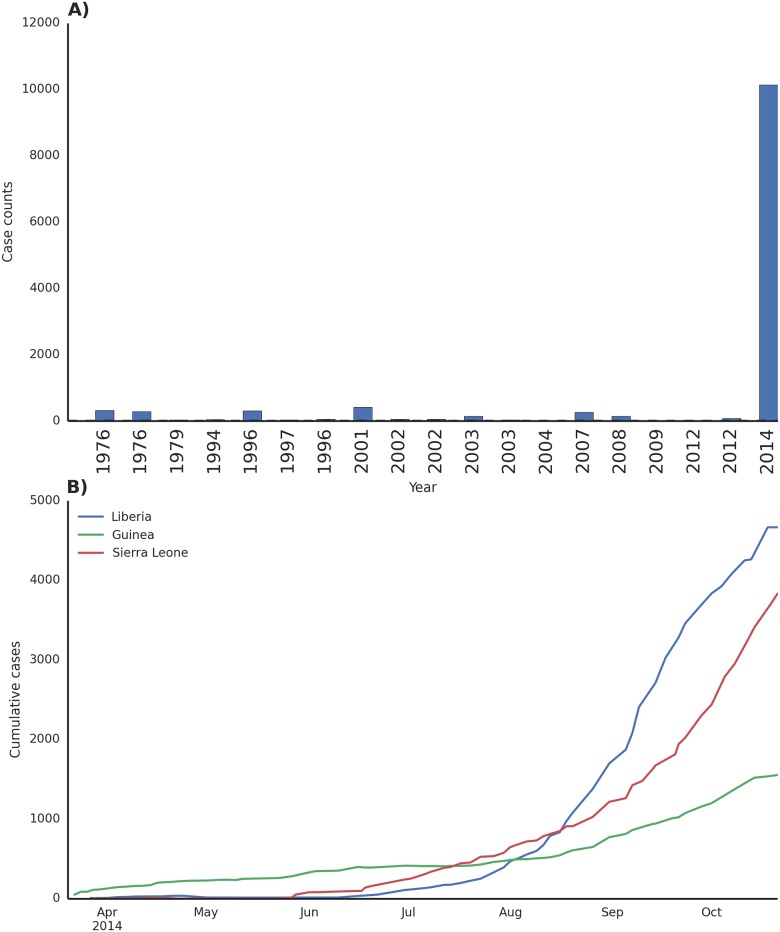
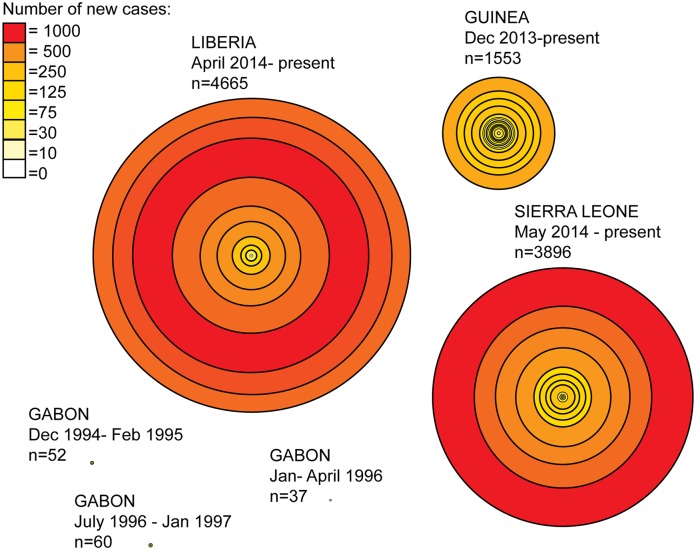
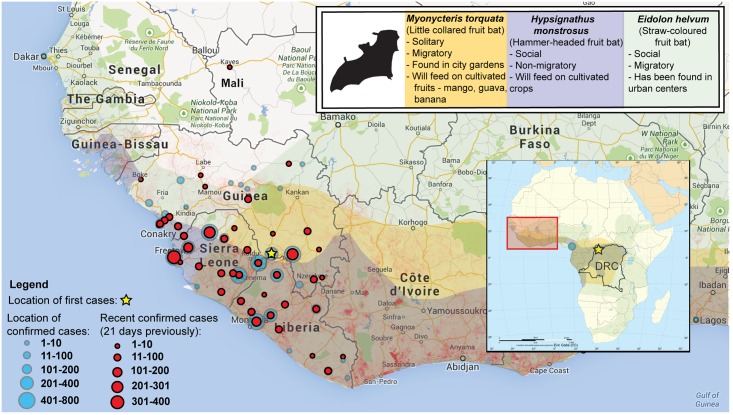
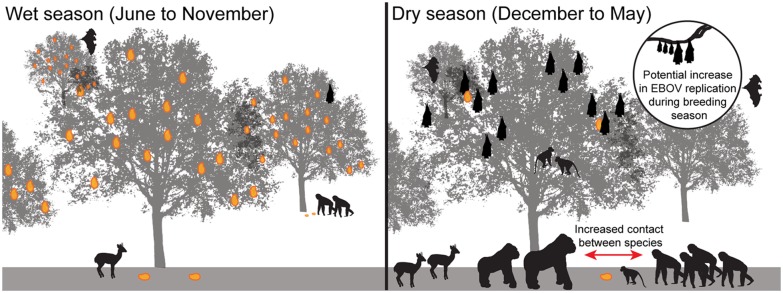
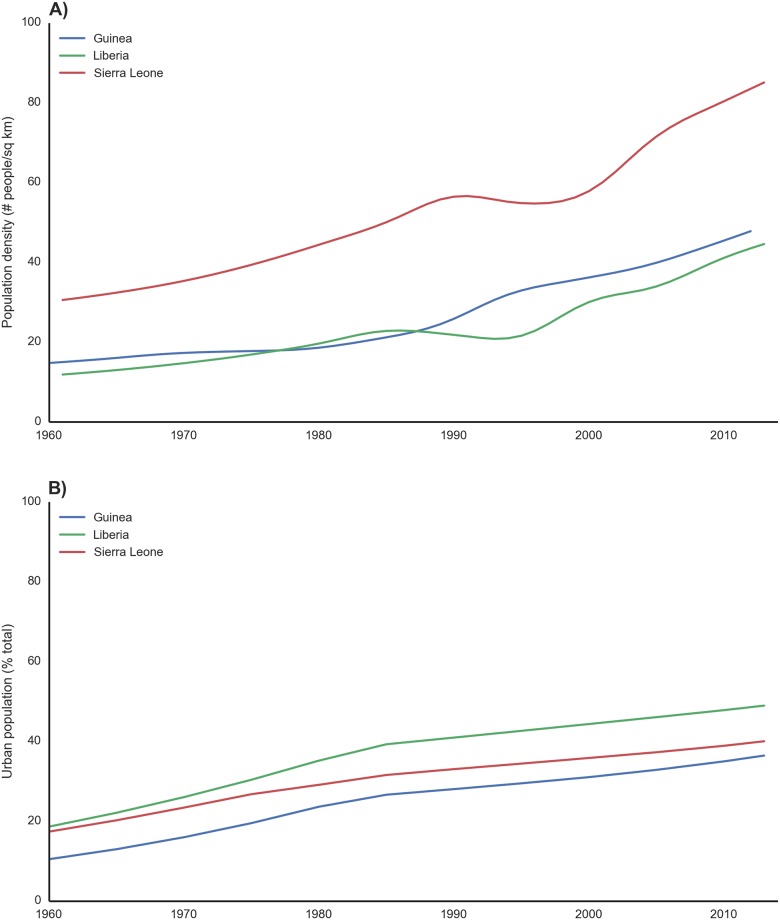
An Ebola outbreak of unprecedented scope emerged in West Africa in December 2013 and presently continues unabated in the countries of Guinea, Sierra Leone, and Liberia. Ebola is not new to Africa, and outbreaks have been confirmed as far back as 1976. The current West African Ebola outbreak is the largest ever recorded and differs dramatically from prior outbreaks in its duration, number of people affected, and geographic extent. The emergence of this deadly disease in West Africa invites many questions, foremost among these: why now, and why in West Africa? Here, we review the sociological, ecological, and environmental drivers that might have influenced the emergence of Ebola in this region of Africa and its spread throughout the region. Containment of the West African Ebola outbreak is the most pressing, immediate need. A comprehensive assessment of the drivers of Ebola emergence and sustained human-to-human transmission is also needed in order to prepare other countries for importation or emergence of this disease. Such assessment includes identification of country-level protocols and interagency policies for outbreak detection and rapid response, increased understanding of cultural and traditional risk factors within and between nations, delivery of culturally embedded public health education, and regional coordination and collaboration, particularly with governments and health ministries throughout Africa. Public health education is also urgently needed in countries outside of Africa in order to ensure that risk is properly understood and public concerns do not escalate unnecessarily. To prevent future outbreaks, coordinated, multiscale, early warning systems should be developed that make full use of these integrated assessments, partner with local communities in high-risk areas, and provide clearly defined response recommendations specific to the needs of each community.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Bright EA, Coleman PR, Rose AN, Urban ML (2012) LandScan 2011. 2011 ed. Oak Ridge, TN: Oak Ridge National Laboratory.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
