

Risk of community-acquired pneumonia with outpatient proton-pump inhibitor therapy: a systematic review and meta-analysis
- PMID: 26042842
- PMCID: PMC4456166
- DOI: 10.1371/journal.pone.0128004
Risk of community-acquired pneumonia with outpatient proton-pump inhibitor therapy: a systematic review and meta-analysis
Abstract
Background: Proton-pump inhibitors (PPIs) are among the most frequently prescribed medications. Community-acquired pneumonia (CAP) is a common cause of morbidity, mortality and healthcare spending. Some studies suggest an increased risk of CAP among PPI users. We conducted a systematic review and meta-analysis to determine the association between outpatient PPI therapy and risk of CAP in adults.
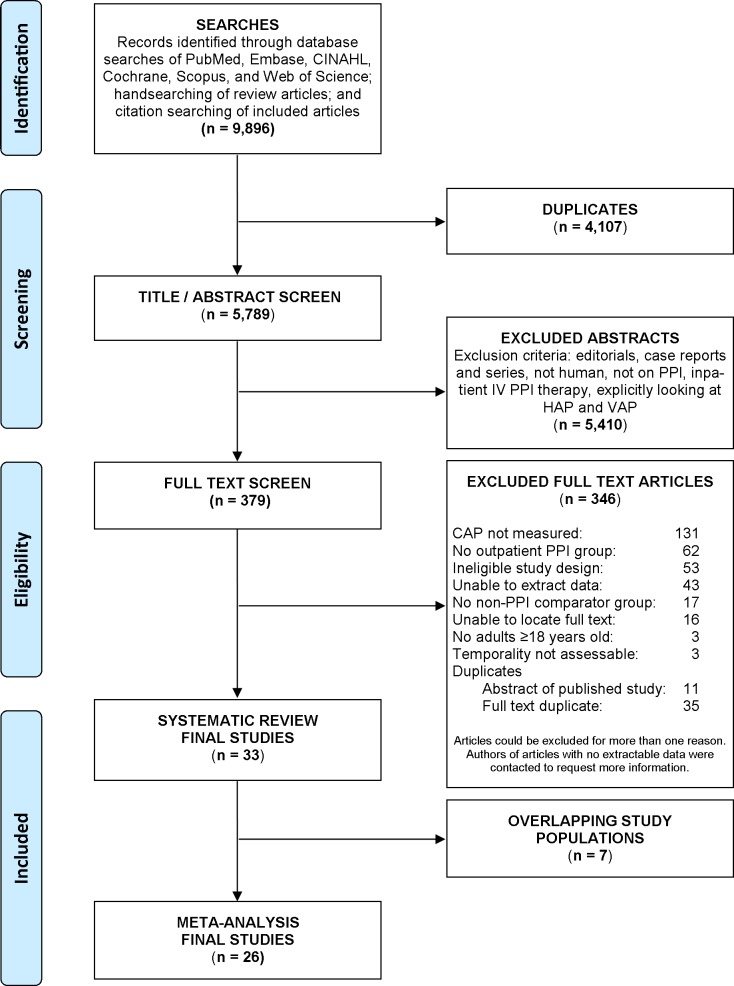
Methods: We conducted systematic searches of MEDLINE, EMBASE, CINAHL, Cochrane Central Register of Controlled Trials, Scopus and Web of Science on February 3, 2014. Case-control studies, case-crossover, cohort studies and randomized controlled trials reporting outpatient PPI exposure and CAP diagnosis for patients ≥18 years old were eligible. Our primary outcome was the association between CAP and PPI therapy. A secondary outcome examined the risk of hospitalization for CAP and subgroup analyses evaluated the association between PPI use and CAP among patients of different age groups, by different PPI doses, and by different durations of PPI therapy.
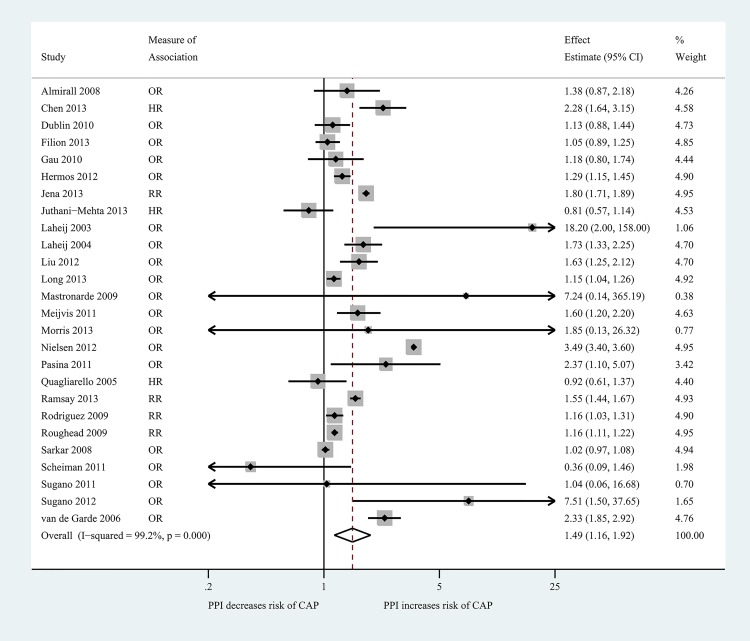
Results: Systematic review of 33 studies was performed, of which 26 studies were included in the meta-analysis. These 26 studies included 226,769 cases of CAP among 6,351,656 participants. We observed a pooled risk of CAP with ambulatory PPI therapy of 1.49 (95% CI 1.16, 1.92; I2 99.2%). This risk was increased during the first month of therapy (OR 2.10; 95% CI 1.39, 3.16), regardless of PPI dose or patient age. PPI therapy also increased risk for hospitalization for CAP (OR 1.61; 95% CI: 1.12, 2.31).
Discussion: Outpatient PPI use is associated with a 1.5-fold increased risk of CAP, with the highest risk within the first 30 days after initiation of therapy. Providers should be aware of this risk when considering PPI use, especially in cases where alternative regimens may be available or the benefits of PPI use are uncertain.
Conflict of interest statement
Figures
References
-
- Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America. 2007;44 Suppl 2:S27–72. Epub 2007/02/06. 10.1086/511159 . - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
