

Reactivity of routine HIV antibody tests in children who initiated antiretroviral therapy in early infancy as part of the Children with HIV Early Antiretroviral Therapy (CHER) trial: a retrospective analysis
- PMID: 26043884
- PMCID: PMC4529673
- DOI: 10.1016/S1473-3099(15)00087-0
Reactivity of routine HIV antibody tests in children who initiated antiretroviral therapy in early infancy as part of the Children with HIV Early Antiretroviral Therapy (CHER) trial: a retrospective analysis
Abstract
Background: Early antiretroviral therapy (ART) and virological suppression can affect evolving antibody responses to HIV infection. We aimed to assess frequency and predictors of seronegativity in infants starting early ART.
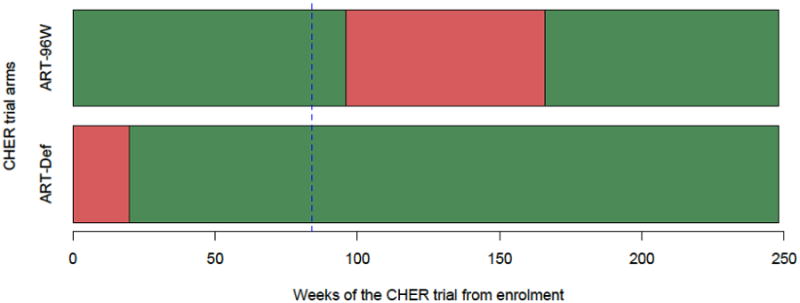
Methods: We compared HIV antibody results between two of three treatment groups of the Children with HIV Early Antiretroviral Therapy (CHER) trial, done from July, 2005, until July, 2011, in which infants with HIV infection aged 5·7-12·0 weeks with a percentage of CD4-positive T lymphocytes of at least 25% were randomly assigned to immediate ART for 96 weeks (ART-96W) or deferred ART until clinical or immunological progression (ART-Def). We measured antibody from all available stored samples for ART-96W and ART-Def at trial week 84 using three assays: fourth-generation enzyme immunoassay HIV antigen-antibody combination, HIV-1 and HIV-2 rapid antibody test, and quantitative anti-gp120 IgG ELISA. We also assessed odds of seropositivity with respect to age of ART initiation and cumulative viral load. The CHER trial was registered with ClinicalTrials.gov, number NCT00102960.
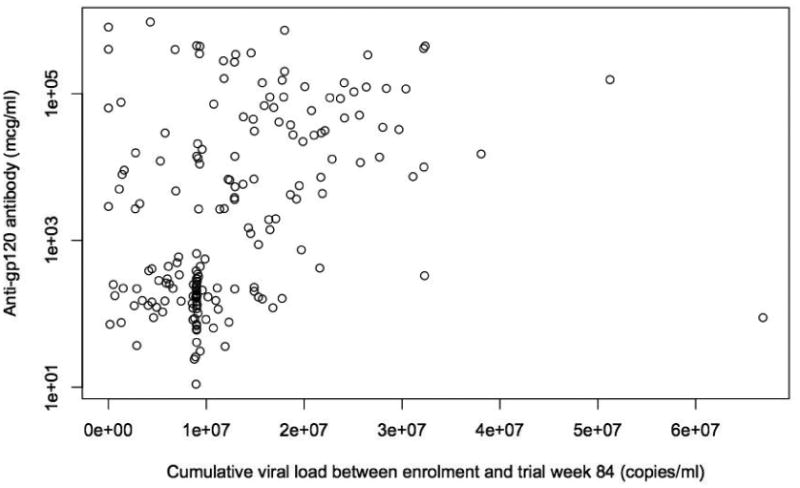
Findings: The median age of the infants from when samples were taken (184 samples from 268 infants) was 92 weeks (IQR 90·6-93·4). More specimens from the ART-96W group were seronegative than from the ART-Def group by enzyme immunoassay (ART-96W 49 [46%] of 107 vs ART-Def eight [11%] of 75; p<0·0001) and rapid antibody test (54 [53%] of 101 vs eight [11%] of 74; p<0·0001). Median anti-gp120 IgG concentration was lower in the ART-96W group (230 μg/μL [IQR 133-13 129]) than in the ART-Def group (6870 μg/μL [1706-53 645]; p<0·0001). If ART was started between 12 and 24 weeks of age, odds of seropositivity were increased 13·7 times (95% CI 3·1-60·2; p=0·001) compared with starting it between 0 and 12 weeks. All children starting ART aged older than 24 weeks were seropositive. Cumulative viral load to week 84 correlated with anti-gp120 IgG concentrations (coefficient 0·54; p<0·0001) and increased odds of seropositivity (odds ratio 1·59 [95% CI 1·1-2·3]) adjusted for ART initiation age.
Interpretation: About half of children starting ART before 12 weeks of age were HIV seronegative by almost 2 years of age. HIV antibody tests cannot be used to reconfirm HIV diagnosis in children starting early ART. Long-term effects of seronegativity need further study. Clear guidelines are needed for retesting alongside improved diagnostic tests.
Funding: Wellcome Trust, Medical Research Council, and National Institutes of Health.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Figures


Comment in
-
The downside of success: confirmation of HIV infection in early treated children.Lancet Infect Dis. 2015 Jul;15(7):751-2. doi: 10.1016/S1473-3099(15)00086-9. Epub 2015 Jun 1. Lancet Infect Dis. 2015. PMID: 26043883 No abstract available.
References
-
- Palasanthiran P, et al. Decay of transplacental human immunodeficiency virus type 1 antibodies in neonates and infants. The Journal of infectious diseases. 1994;170(6):1593–6. - PubMed
-
- Hospitalization of children born to human immunodeficiency virus-infected women in Europe. The European Collaborative Study. The Pediatric infectious disease journal. 1997;16(12):1151–6. - PubMed
-
- Hainaut M, et al. Seroreversion in children infected with HIV type 1 who are treated in the first months of life is not a rare event. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America. 2005;41(12):1820–1. - PubMed
-
- Vigano A, et al. Failure to eradicate HIV despite fully successful HAART initiated in the first days of life. The Journal of pediatrics. 2006;148(3):389–91. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
