

Lambl's Excrescences: Association with Cerebrovascular Disease and Pathogenesis
- PMID: 26044080
- PMCID: PMC4592773
- DOI: 10.1159/000381906
Lambl's Excrescences: Association with Cerebrovascular Disease and Pathogenesis
Abstract
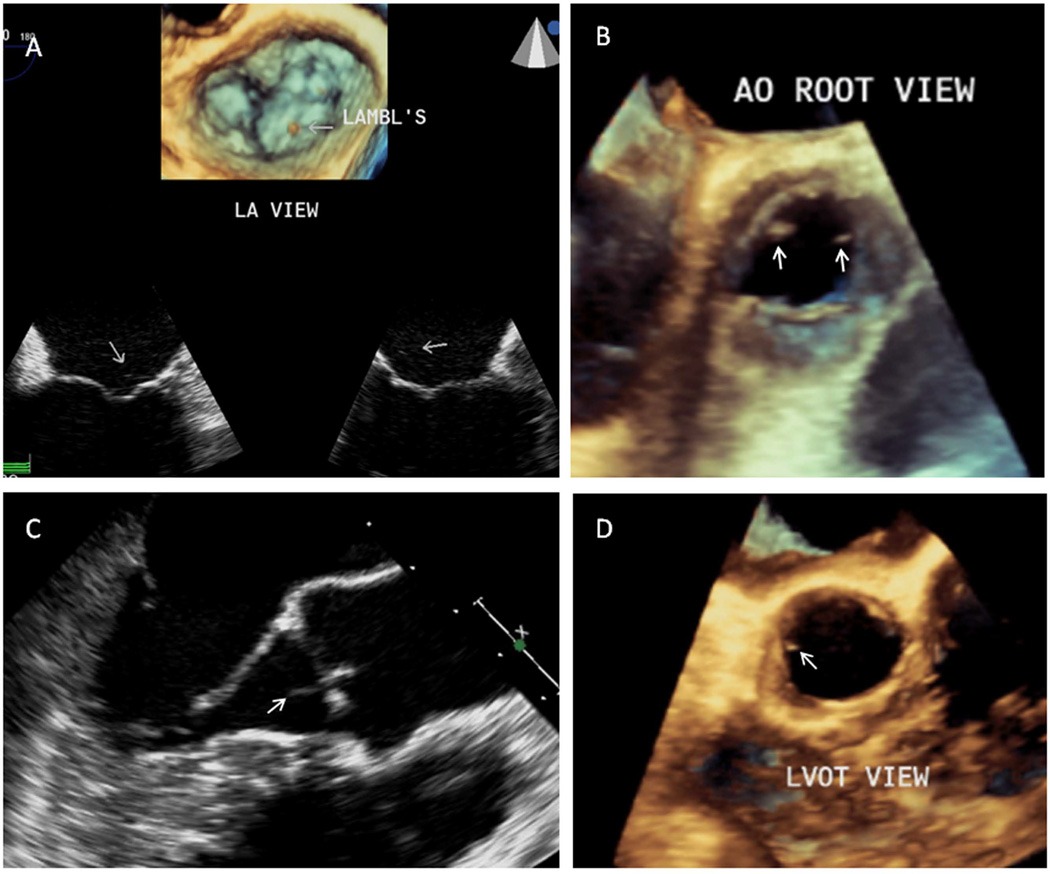
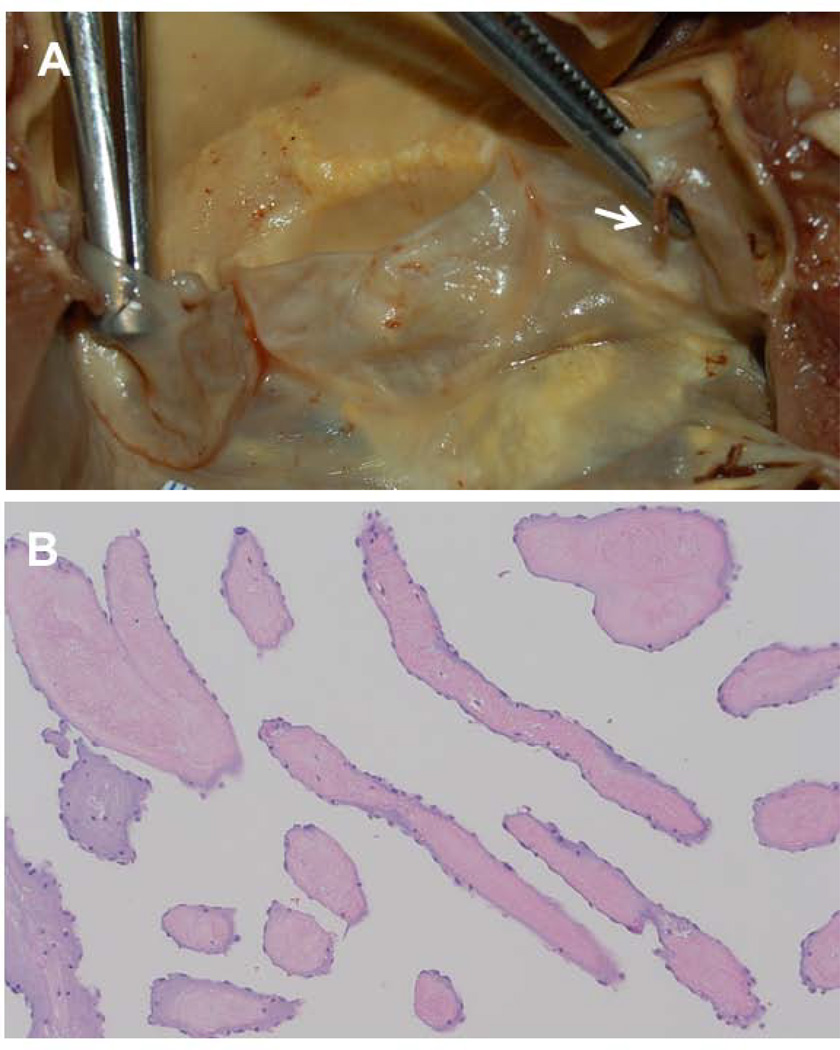
Background: Lambl's excrescences (LEx) are detected by transesophageal echocardiography (TEE) and are characterized as thin, elongated, and hypermobile structures located at the leaflets' coaptation point of the heart valves. The association of LEx with cerebrovascular disease (CVD) is still undefined and yet patients with LEx and suspected CVD receive unproven effective antiplatelet or anticoagulant therapy or even undergo valve surgery. Also, the association of LEx with aging and atherogenic, inflammatory, or thrombogenic parameters has not been reported.
Methods: Seventy-seven patients with systemic lupus erythematosus (SLE) (71 women, age 37 ± 12 years) and 26 age- and sex-matched healthy controls (22 women, age 34 ± 11 years) prospectively underwent routine history and physical exam, transcranial Doppler, brain MRI, TEE, carotid duplex, and clinical and laboratory evaluations of atherogenesis, inflammation, platelet activity, coagulation, and fibrinolysis. Subjects without stroke/TIA on enrollment (with and without LEx) had a median follow-up of 57 months.
Results: On enrollment, 33 (43%) of 77 patients had CVD manifested as acute stroke/TIA (23 patients), cerebromicroembolism by transcranial Doppler (17 patients), or cerebral infarcts by MRI (14 patients). Mitral or aortic valve LEx were equally frequent in healthy controls (46%) as in patients with and without any CVD (39 and 43%), stroke/TIA (35 and 43%), cerebromicroembolism (41 and 42%), or cerebral infarcts (36 and 43%) (all p ≥ 0.72). Also, other mechanisms for CVD other than LEx such as Libman-Sacks vegetations, patent foramen ovale or interatrial septal aneurysm, aortic or carotid atherosclerosis, or thrombogenesis were found in ≥94% of patients with CVD. In addition, 36 subjects with and 44 without LEx had similar low incidence of stroke/TIA (1 (1.3%) and 2 (2.5%), respectively, p = 1.0) during follow-up. Finally, LEx were not associated with aging, atherogenic risk factors, atherosclerosis, inflammation, or thrombogenesis.
Conclusions: In this study, LEx are similarly prevalent in healthy controls and SLE patients, are not associated with CVD, and are not associated with pathogenic risk factors. Therefore, the study findings suggest that LEx may not be cardioembolic substrates, may not represent pathologic valve structures, and may not require therapy.
Conflict of interest statement
None of the authors has conflicts of interest to disclose.
Figures
References
-
- Lambl VA. Papillare excrescenzen und der semilunar-klappe der aorta. Wien Med Wochenschr. 1856;16:244–250.
-
- Lee RJ, Bartzokis T, Yeoh T, Grogin HR, Choi D, Schnittger I. Enhanced detection of intracardiac sources of cerebral emboli by transesophageal echocardiography. Stroke. 1991;22:734–739. - PubMed
-
- Freedberg RS, Goodkin GM, Perez JL, Tunick PA, Kronzon I. Valve strands are strongly associated with systemic embolization: a transesophageal echocardiographic study. J Am Coll Cardiol. 1995;26:1709–1712. - PubMed
-
- Homma S, Di Tullio MR, Sciacca RR, Sacco RL, Mohr JP. Effect of aspirin and warfarin therapy in stroke patients with valvular strands. PICSS Investigators. Stroke. 2004;35:1436–1442. - PubMed
-
- Roldan CA, Shively BK, Crawford MH. Valve Excrescences: Prevalence, evolution and risk for cardioembolism. J Am Coll Cardiol. 1998;30:1308–1314. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
