

The spectrum of epidemiology underlying sudden cardiac death
- PMID: 26044246
- PMCID: PMC4929621
- DOI: 10.1161/CIRCRESAHA.116.304521
The spectrum of epidemiology underlying sudden cardiac death
Abstract
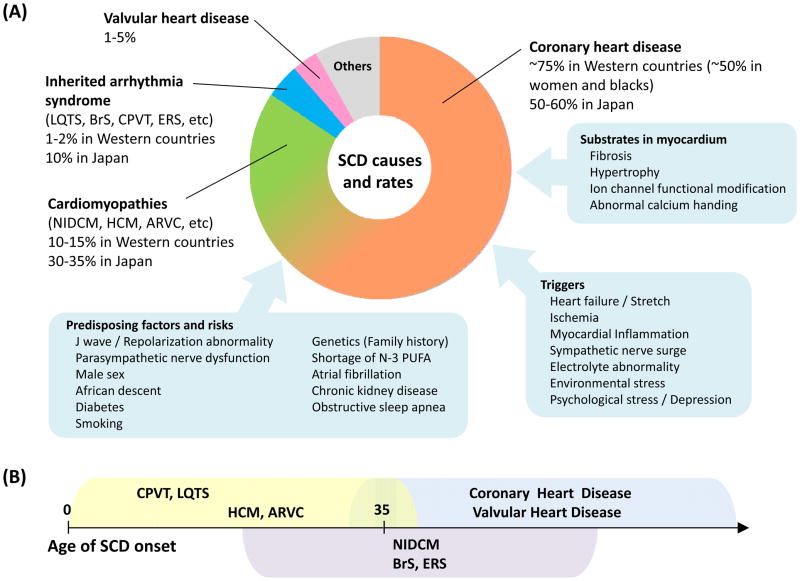
Sudden cardiac death (SCD) from cardiac arrest is a major international public health problem accounting for an estimated 15%-20% of all deaths. Although resuscitation rates are generally improving throughout the world, the majority of individuals who experience a sudden cardiac arrest will not survive. SCD most often develops in older adults with acquired structural heart disease, but it also rarely occurs in the young, where it is more commonly because of inherited disorders. Coronary heart disease is known to be the most common pathology underlying SCD, followed by cardiomyopathies, inherited arrhythmia syndromes, and valvular heart disease. During the past 3 decades, declines in SCD rates have not been as steep as for other causes of coronary heart disease deaths, and there is a growing fraction of SCDs not due to coronary heart disease and ventricular arrhythmias, particularly among certain subsets of the population. The growing heterogeneity of the pathologies and mechanisms underlying SCD present major challenges for SCD prevention, which are magnified further by a frequent lack of recognition of the underlying cardiac condition before death. Multifaceted preventative approaches, which address risk factors in seemingly low-risk and known high-risk populations, will be required to decrease the burden of SCD. In this Compendium, we review the wide-ranging spectrum of epidemiology underlying SCD within both the general population and in high-risk subsets with established cardiac disease placing an emphasis on recent global trends, remaining uncertainties, and potential targeted preventive strategies.
Keywords: cardiomyopathies; coronary disease; death, sudden, cardiac; epidemiology.
© 2015 American Heart Association, Inc.
Figures
References
-
- Lopshire JC, Zipes DP. Sudden cardiac death: Better understanding of risks, mechanisms, and treatment. Circulation. 2006;114:1134–1136. - PubMed
-
- Hinkle LE, Jr, Thaler HT. Clinical classification of cardiac deaths. Circulation. 1982;65:457–464. - PubMed
-
- Albert CM, Chae CU, Grodstein F, Rose LM, Rexrode KM, Ruskin JN, Stampfer MJ, Manson JE. Prospective study of sudden cardiac death among women in the United States. Circulation. 2003;107:2096–2101. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
