

Assessment of clinical findings, tryptase levels, and bone marrow histopathology in the management of pediatric mastocytosis
- PMID: 26044856
- PMCID: PMC4984538
- DOI: 10.1016/j.jaci.2015.04.024
Assessment of clinical findings, tryptase levels, and bone marrow histopathology in the management of pediatric mastocytosis
Abstract
Background: The management of children with pediatric mastocytosis poses a challenge. This is because there is limited information as to the application of clinical and laboratory findings and bone marrow histopathology as they relate to medical intervention and communication.
Objective: We sought to examine clinical aspects of pediatric mastocytosis in relationship to serum tryptase levels and bone marrow pathology to provide practical guidance for management.
Methods: Between 1986 and 2012, 105 children were evaluated at the National Institutes of Health. Organomegaly was confirmed by means of ultrasound. Baseline tryptase levels and at least 1 subsequent tryptase measurement was available in 84 and 37 of these children, respectively. Fifty-three children underwent a bone marrow examination. These data were used to examine relationships between clinical findings, tryptase levels, and marrow histopathology.
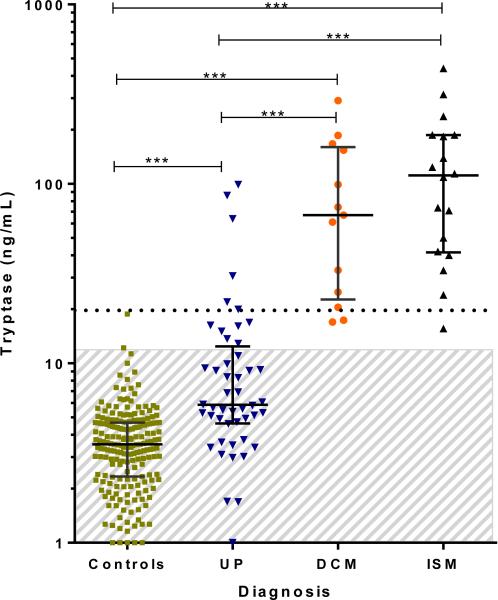
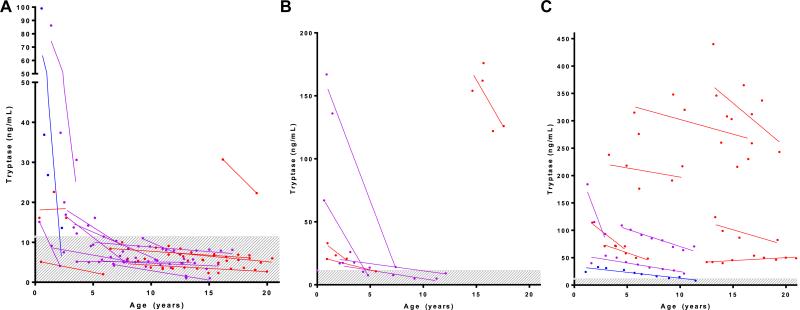
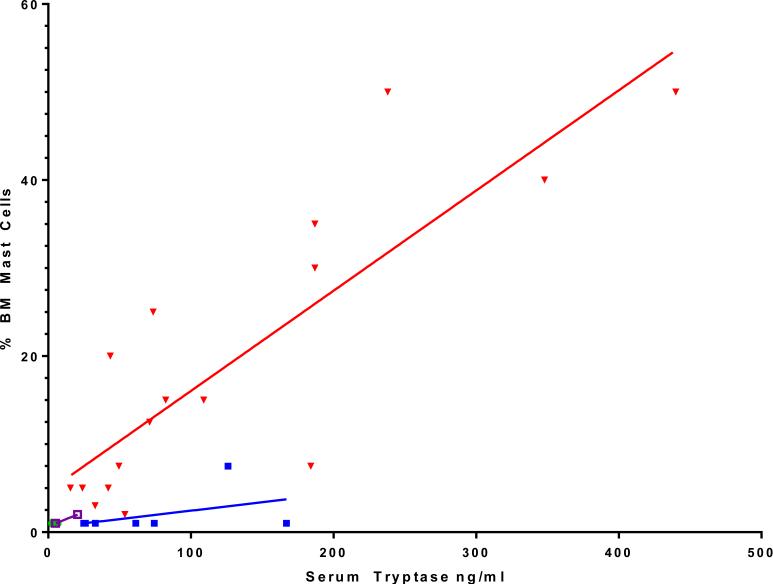
Results: In patients with high tryptase levels and severe mediator symptoms, all with organomegaly had systemic disease, and none without organomegaly had systemic disease. Serum tryptase levels differed significantly between patients with urticaria pigmentosa and those with diffuse cutaneous (P < .0001) and systemic mastocytosis (P < .0001) and in all 3 categories versus control subjects (P < .0001). Tryptase levels and symptoms decreased over time in most patients, and tryptase levels correlated with bone marrow mast cell burden in patients with systemic mastocytosis (P < .0001). There was a significant relationship between clinical resolution and the percentage decrease in tryptase levels (P = .0014).
Conclusions: The majority of children experienced major or complete disease resolution (57%), whereas the remainder exhibited partial improvement. Organomegaly was a strong indicator of systemic disease. Serum tryptase levels furthered classification and reflected clinicopathologic findings, while sequential tryptase measurements were useful in supplementing clinical judgment as to disease course.
Keywords: Mast cells; bone marrow examination; cutaneous mastocytosis; diffuse cutaneous mastocytosis; mastocytosis; tryptase; urticaria pigmentosa.
Published by Elsevier Inc.
Figures
References
-
- Amon U, Hartmann K, Horny HP, Nowak A. Mastocytosis—an update. J Dtsch Dermatol Ges. 2010;8:695–712. - PubMed
-
- Caplan R. The natural course of urticaria pigmentosa. Arch Dermatol. 1963;87:146–57. - PubMed
-
- Brockow K, Akin C, Huber M, Metcalfe DD. Assessment of the extent of cutaneous involvement in children and adults with mastocytosis: relationship to symptomatology, tryptase levels, and bone marrow pathology. J Am Acad Dermatol. 2003;48:508–16. - PubMed
-
- Lange M, Niedoszytko M, Renke J, Glen J, Nedoszytko B. Clinical aspects of paediatric mastocytosis: a review of 101 cases. J Eur Acad Dermatol Venereol. 2013;27:97–102. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
