

Pulmonary Arterial Capacitance Is an Important Predictor of Mortality in Heart Failure With a Preserved Ejection Fraction
- PMID: 26046840
- PMCID: PMC4536851
- DOI: 10.1016/j.jchf.2015.01.013
Pulmonary Arterial Capacitance Is an Important Predictor of Mortality in Heart Failure With a Preserved Ejection Fraction
Abstract
Objectives: The purpose of this study was to determine the predictors of mortality in patients with pulmonary hypertension (PH) associated with heart failure with preserved ejection fraction (HFpEF).
Background: PH is commonly associated with HFpEF. The predictors of mortality for patients with these conditions are not well characterized.
Methods: In a prospective cohort of patients with right heart catheterization, we identified 73 adult patients who had pulmonary hypertension due to left heart disease (PH-LHD) associated with HFpEF (left ventricular ejection fraction ≥50% by echocardiography); hemodynamically defined as a mean pulmonary artery pressure ≥25 mm Hg and pulmonary artery wedge pressure >15 mm Hg. PH severity was classified according to the diastolic pressure gradient (DPG). Cox proportional hazards ratios were used to estimate the associations between clinical variables and mortality. Receiver-operating characteristic curves were used to evaluate the ability of hemodynamic measurements to predict mortality.
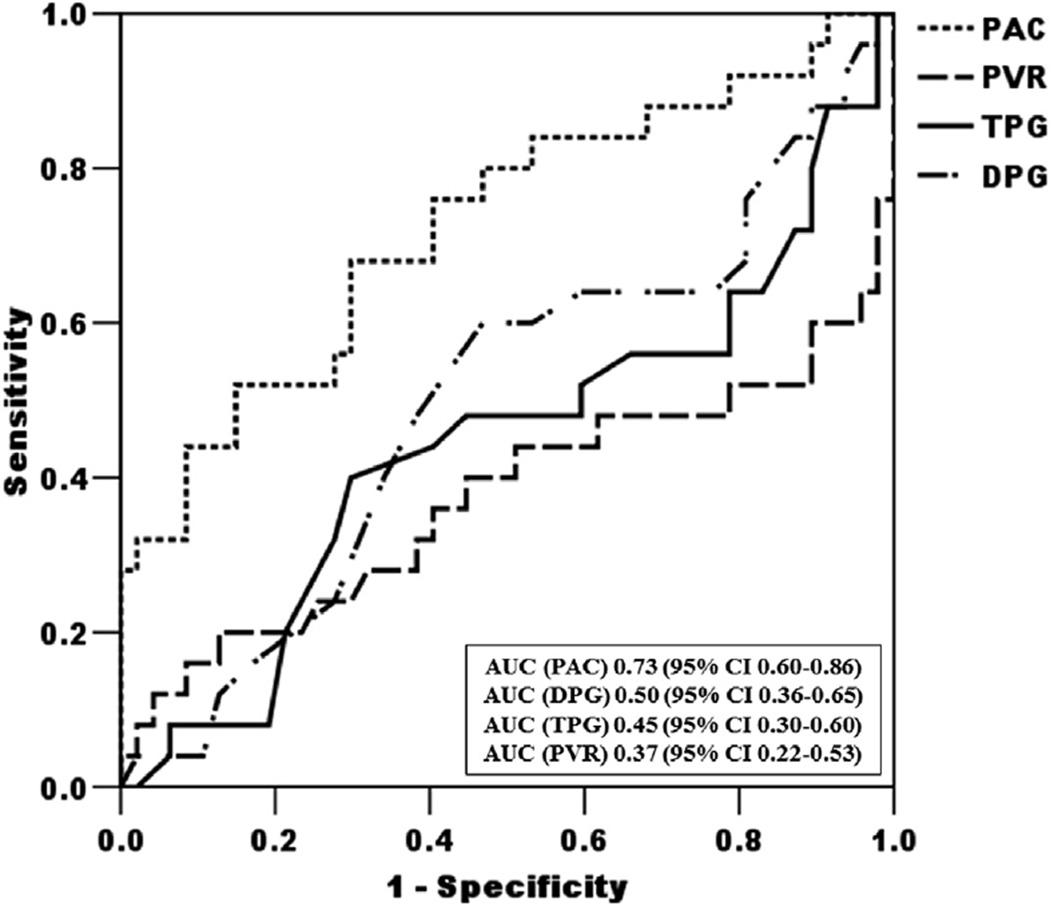
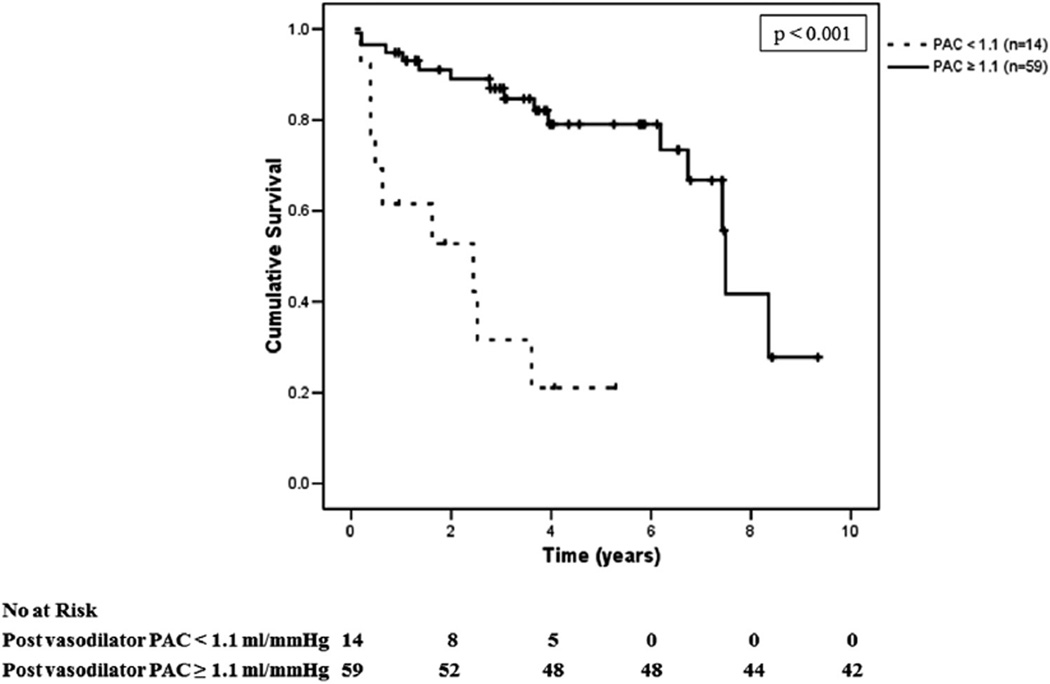
Results: The mean age for study subjects was 69 ± 12 years and 74% were female. Patients classified as having combined post-capillary PH and pre-capillary PH (DPG ≥7) were not at increased risk of death as compared to patients with isolated post-capillary PH (DPG <7). A baseline pulmonary arterial capacitance (PAC) of <1.1 ml/mm Hg was 91% sensitive in predicting mortality, with better discriminatory ability than DPG, transpulmonary gradient, or pulmonary vascular resistance (area under the curve of 0.73, 0.50, 0.45, and 0.37, respectively). Fifty-seven subjects underwent acute vasoreactivity testing with inhaled nitric oxide. Acute vasodilator response by the Rich or Sitbon criteria was not associated with improved survival.
Conclusions: PAC is the best predictor of mortality in our cohort and may be useful in describing phenotypic subgroups among those with PH-LHD associated with HFpEF. Acute vasodilator testing did not predict outcome in our cohort but needs to be further investigated.
Keywords: heart failure with preserved ejection fraction; pulmonary heart disease; survival; vasodilation.
Copyright © 2015 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
In Search of New Targets and Endpoints in Heart Failure With Preserved Ejection Fraction.JACC Heart Fail. 2015 Jun;3(6):475-477. doi: 10.1016/j.jchf.2015.02.007. JACC Heart Fail. 2015. PMID: 26046841 No abstract available.
-
The Diastolic Pressure Gradient Does Not-and Should Not-Predict Outcomes.JACC Heart Fail. 2015 Oct;3(10):845. doi: 10.1016/j.jchf.2015.06.008. JACC Heart Fail. 2015. PMID: 26450004 No abstract available.
-
Reply: The Diastolic Pressure Gradient Does Not-and Should Not-Predict Outcomes.JACC Heart Fail. 2015 Oct;3(10):846. doi: 10.1016/j.jchf.2015.07.007. JACC Heart Fail. 2015. PMID: 26450005 No abstract available.
References
-
- Hill NS, Preston I, Roberts K. Defining the phenotypes for pulmonary hypertension associated with diastolic heart failure. Circ Heart Fail. 2011;4:238–240. - PubMed
-
- Hogg K, Swedberg K, McMurray J. Heart failure with preserved left ventricular systolic function; epidemiology, clinical characteristics, and prognosis. J Am Coll Cardiol. 2004;43:317–327. - PubMed
-
- Damy T, Goode KM, Kallvikbacka-Bennett A, et al. Determinants and prognostic value of pulmonary arterial pressure in patients with chronic heart failure. Eur Heart J. 2010;31:2280–2290. - PubMed
-
- Galie N, Hoeper MM, Humbert M, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension: the Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT) Eur Heart J. 2009;30:2493–2537. - PubMed
-
- McLaughlin VV, Archer SL, Badesch DB, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association developed in collaboration with the American College of Chest Physicians; American Thoracic Society, Inc.; and the Pulmonary Hypertension Association. J Am Coll Cardiol. 2009;53:1573–1619. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
