

Evaluation of Microscopic Observation Drug Susceptibility (MODS) and the string test for rapid diagnosis of pulmonary tuberculosis in HIV/AIDS patients in Bolivia
- PMID: 26047953
- PMCID: PMC4458042
- DOI: 10.1186/s12879-015-0966-0
Evaluation of Microscopic Observation Drug Susceptibility (MODS) and the string test for rapid diagnosis of pulmonary tuberculosis in HIV/AIDS patients in Bolivia
Abstract
Background: Tuberculosis (TB) is the most common opportunistic infection and the leading cause of death in HIV-positive people worldwide. Diagnosing TB is difficult, and is more challenging in resource-scarce settings where culture-based diagnostic methods rely on poorly sensitive smear microscopy by Ziehl-Neelsen stain (ZN).
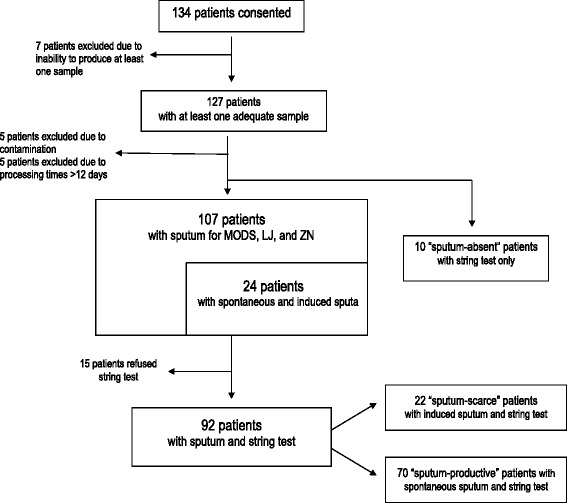
Methods: We performed a cross-sectional study examining the diagnostic utility of Microscopic Observation Drug Susceptibility liquid culture (MODS) versus traditional Ziehl-Neelsen staining (ZN) and Lowenstein Jensen culture (LJ) of pulmonary tuberculosis (TB) and multidrug-resistant tuberculosis (MDRTB) in HIV-infected patients in Bolivia. For sputum scarce individuals we assessed the value of the string test and induced sputum for TB diagnosis. The presence of Mycobacterium tuberculosis (Mtb) in the sputum of 107 HIV-positive patients was evaluated by ZN, LJ, and MODS. Gastric secretion samples obtained by the string test were evaluated by MODS in 102 patients.
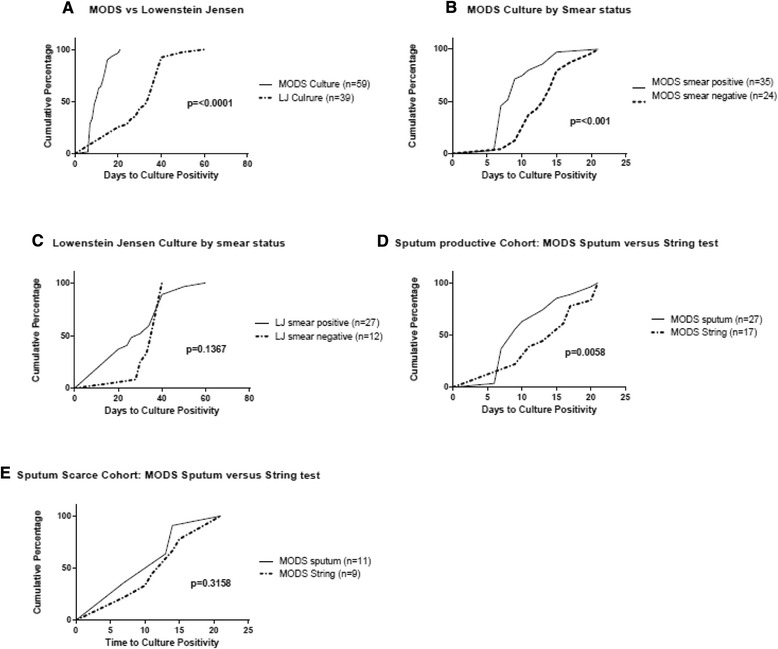
Results: The TB-HIV co-infection rate of HIV patients with respiratory symptoms by sputum sample was 45 % (48/107); 46/48 (96 %) were positive by MODS, 38/48 (79 %) by LJ, and 30/48 (63 %) by ZN. The rate of MDRTB was 9 % (4/48). Median time to positive culture was 10 days by MODS versus 34 days by LJ (p < 0.0001). In smear-negative patients, MODS detected TB in 17/18 patients, compared to 11/18 by LJ (94.4 % vs 61.0 %, p = 0.03 %). In patients unable to produce a sputum sample without induction, the string test cultured by MODS yielded Mtb in of 9/11 (82 %) TB positive patients compared to 11/11 (100 %) with induced sputum. Of the 10 patients unable to produce a sputum sample, 4 were TB-positive by string test.
Conclusion: MODS was faster and had a higher Mtb detection yield compared to LJ, with a greater difference in yield between the two in smear-negative patients. The string test is a valuable diagnostic technique for HIV sputum-scarce or sputum-absent patients, and should be considered as an alternative test to induced sputum to obtain sample for Mtb in resource-limited settings. Nine percent of our TB+ patients had MDRTB, which reinforces the need for rapid detection with direct drug susceptibility testing in HIV patients in Bolivia.
Figures
References
-
- World Health Organization: Global tuberculosis report. Geneva; 2014. http://www.who.int/tb/publications/global_report/en/. Accessed 31 May 2015.
-
- Ministerio de Salud y Deportes: Programa Nacional de Control de Tuberculosis. Boletín Informativo, Bolivia. 2012. http://snis.minsalud.gob.bo/tuberculosis/Docs/Boletin/Boletin%20TB%20201.... Accessed 31 May 2015.
-
- American Thoracic Society Diagnostic standards and classification of tuberculosis in adults and children. Consensus from an expert panel. Am J Respir CritCare Med. 2000;161:1376. doi: 10.1164/ajrccm.161.4.16141. - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
