

Comparison of zotarolimus- and everolimus-eluting coronary stents: final 5-year report of the RESOLUTE all-comers trial
- PMID: 26047993
- PMCID: PMC4495878
- DOI: 10.1161/CIRCINTERVENTIONS.114.002230
Comparison of zotarolimus- and everolimus-eluting coronary stents: final 5-year report of the RESOLUTE all-comers trial
Abstract
Background: Newer-generation drug-eluting stents that release zotarolimus or everolimus have been shown to be superior to the first-generation drug-eluting stents. However, data comparing long-term safety and efficacy of zotarolimus- (ZES) and everolimus-eluting stents (EES) are limited. RESOLUTE all-comers (Randomized Comparison of a Zotarolimus-Eluting Stent With an Everolimus-Eluting Stent for Percutaneous Coronary Intervention) trial compared these 2 stents and has shown that ZES was noninferior to EES at 12-month for the primary end point of target lesion failure. We report the secondary clinical outcomes at the final 5-year follow-up of this trial.
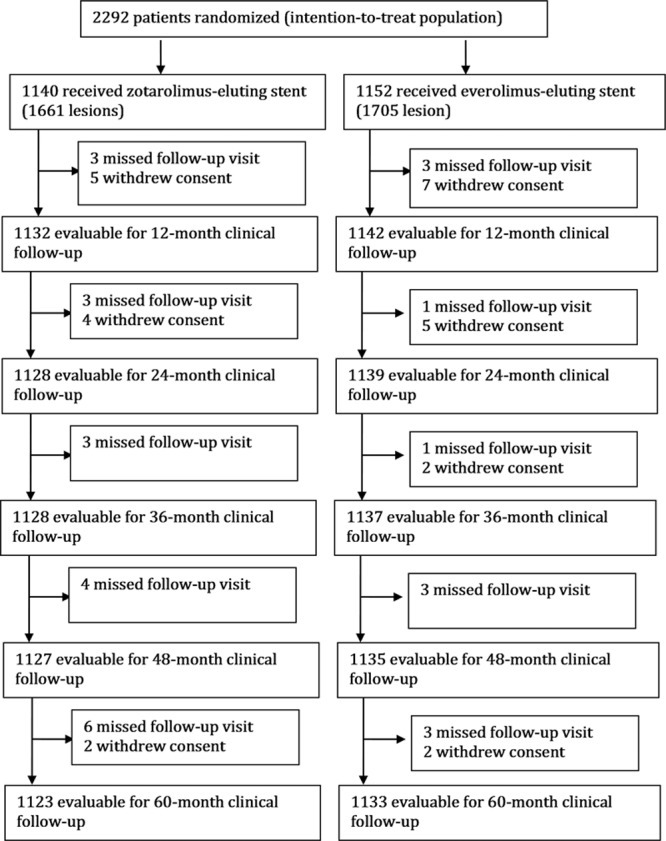
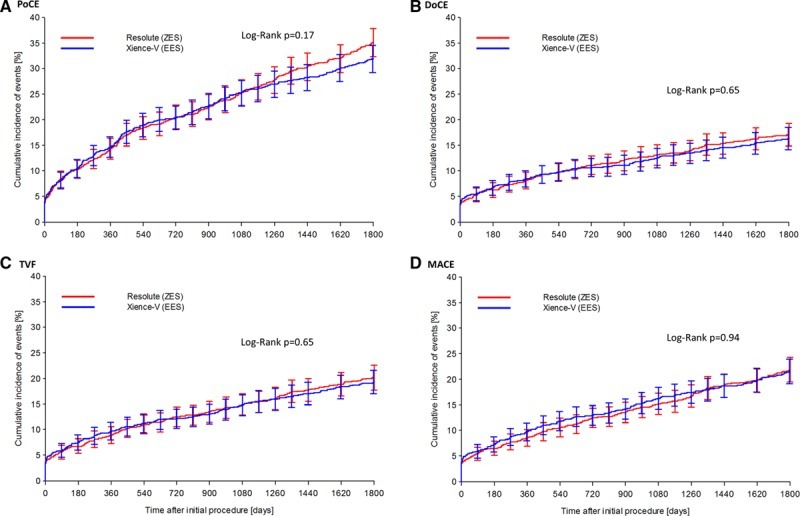
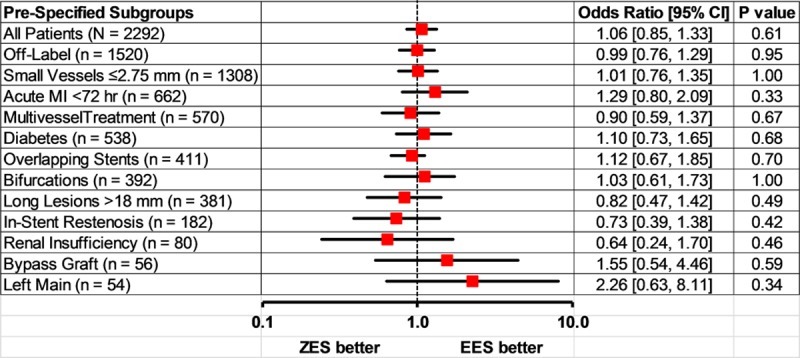
Methods and results: RESOLUTE all-comer clinical study is a prospective, multicentre, randomized, 2-arm, open-label, noninferiority trial with minimal exclusion criteria. Patients (n=2292) were randomly assigned to treatment with either ZES (n=1140) or EES (n=1152). Patient-oriented composite end point (combination of all-cause mortality, myocardial infarction, and any revascularizations), device-oriented composite end point (combination of cardiac death, target vessel myocardial infarction, and clinically indicated target lesion revascularization), and major adverse cardiac events (combination of all-cause death, all myocardial infarction, emergent coronary bypass surgery, or clinically indicated target lesion revascularization) were analyzed at 5-year follow-up. The 2 groups were well-matched at baseline. Five-year follow-up data were available for 98% patients. There were no differences in patient-oriented composite end point (ZES 35.3% versus EES 32.0%, P=0.11), device-oriented composite end point (ZES 17.0% versus EES 16.2%, P=0.61), major adverse cardiac events (ZES 21.9% versus EES 21.6%, P=0.88), and definite/probable stent thrombosis (ZES 2.8% versus EES 1.8%, P=0.12).
Conclusions: At 5-year follow-up, ZES and EES had similar efficacy and safety in a population of patients who had minimal exclusion criteria.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT00617084.
Keywords: drug-eluting stent; everolimus; percutaneous coronary interventions; zotarolimus.
© 2015 The Authors.
Figures
References
-
- de Feyter PJ, de Jaegere PP, Serruys PW. Incidence, predictors, and management of acute coronary occlusion after coronary angioplasty. Am Heart J. 1994;127:643–651. - PubMed
-
- Serruys PW, de Jaegere P, Kiemeneij F, Macaya C, Rutsch W, Heyndrickx G, Emanuelsson H, Marco J, Legrand V, Materne P. A comparison of balloon-expandable-stent implantation with balloon angioplasty in patients with coronary artery disease. Benestent Study Group. N Engl J Med. 1994;331:489–495. doi: 10.1056/NEJM199408253310801. - PubMed
-
- Fischman DL, Leon MB, Baim DS, Schatz RA, Savage MP, Penn I, Detre K, Veltri L, Ricci D, Nobuyoshi M. A randomized comparison of coronary-stent placement and balloon angioplasty in the treatment of coronary artery disease. Stent Restenosis Study Investigators. N Engl J Med. 1994;331:496–501. doi: 10.1056/NEJM199408253310802. - PubMed
-
- Serruys PW, Strauss BH, Beatt KJ, Bertrand ME, Puel J, Rickards AF, Meier B, Goy JJ, Vogt P, Kappenberger L. Angiographic follow-up after placement of a self-expanding coronary-artery stent. N Engl J Med. 1991;324:13–17. doi: 10.1056/NEJM199101033240103. - PubMed
-
- Morice MC, Serruys PW, Sousa JE, Fajadet J, Ban Hayashi E, Perin M, Colombo A, Schuler G, Barragan P, Guagliumi G, Molnàr F, Falotico R RAVEL Study Group. Randomized Study with the Sirolimus-Coated Bx Velocity Balloon-Expandable Stent in the Treatment of Patients with de Novo Native Coronary Artery Lesions. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med. 2002;346:1773–1780. doi: 10.1056/NEJMoa012843. - PubMed
