

Perturbation training to promote safe independent mobility post-stroke: study protocol for a randomized controlled trial
- PMID: 26048054
- PMCID: PMC4456796
- DOI: 10.1186/s12883-015-0347-8
Perturbation training to promote safe independent mobility post-stroke: study protocol for a randomized controlled trial
Abstract
Background: Falls are one of the most common medical complications post-stroke. Physical exercise, particularly exercise that challenges balance, reduces the risk of falls among healthy and frail older adults. However, exercise has not proven effective for preventing falls post-stroke. Falls ultimately occur when an individual fails to recover from a loss of balance. Thus, training to specifically improve reactive balance control could prevent falls. Perturbation training aims to improve reactive balance control by repeatedly exposing participants to postural perturbations. There is emerging evidence that perturbation training reduces fall rates among individuals with neurological conditions, such as Parkinson disease. The primary aim of this work is to determine if perturbation-based balance training can reduce occurrence of falls in daily life among individuals with chronic stroke. Secondary objectives are to determine the effect of perturbation training on balance confidence and activity restriction, and functional balance and mobility.
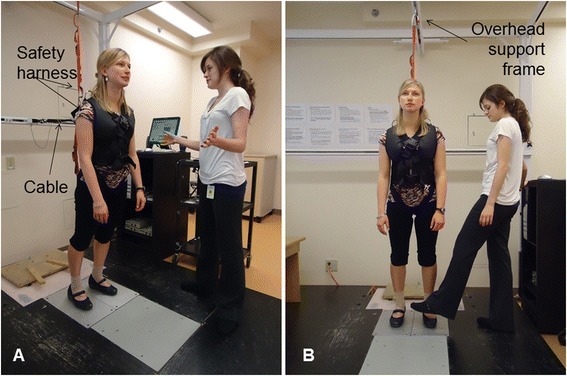
Methods/design: Individuals with chronic stroke will be recruited. Participants will be randomly assigned to one of two groups: 1) perturbation training, or 2) 'traditional' balance training. Perturbation training will involve both manual perturbations (e.g., a push or pull from a physiotherapist), and rapid voluntary movements to cause a loss of balance. Training will occur twice per week for 6 weeks. Participants will record falls and activity for 12 months following completion of the training program. Standardized clinical tools will be used to assess functional balance and mobility, and balance confidence before and after training.
Discussion: Falls are a significant problem for those with stroke. Despite the large body of work demonstrating effective interventions, such as exercise, for preventing falls in other populations, there is little evidence for interventions that prevent falls post-stroke. The proposed study will investigate a novel and promising intervention: perturbation training. If effective, this training has the potential to not only prevent falls, but to also improve safe independent mobility and engagement in daily activities for those with stroke.
Trial registration: Current Controlled Trials: ISRCTN05434601 .
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
